Hematology and Bone Marrow Transplantation, San Raffaele Scientific Institute, Milan, Italy.
Clinic of Infectious Diseases, San Raffaele Scientific Institute, Milan, Italy.
Blood Adv. 2023 May 9;7(9):1621-1634. doi: 10.1182/bloodadvances.2022008226.
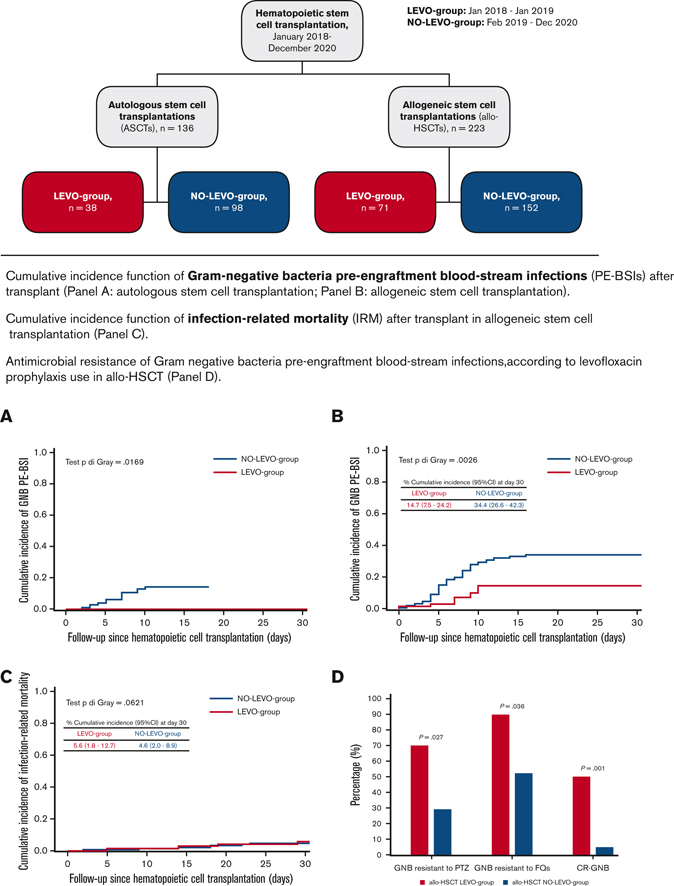
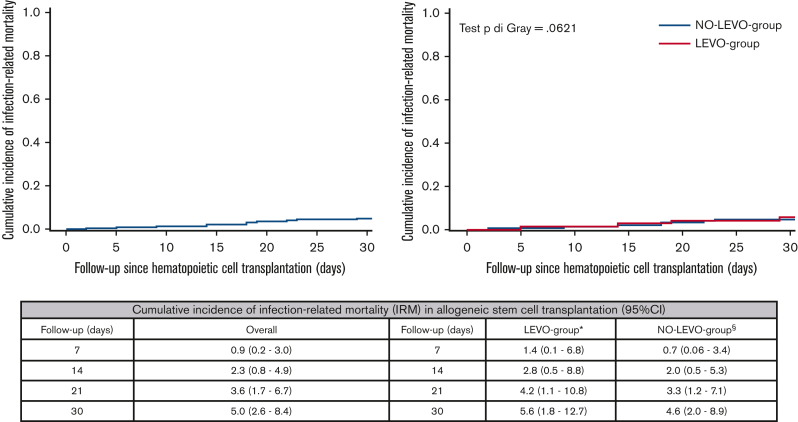
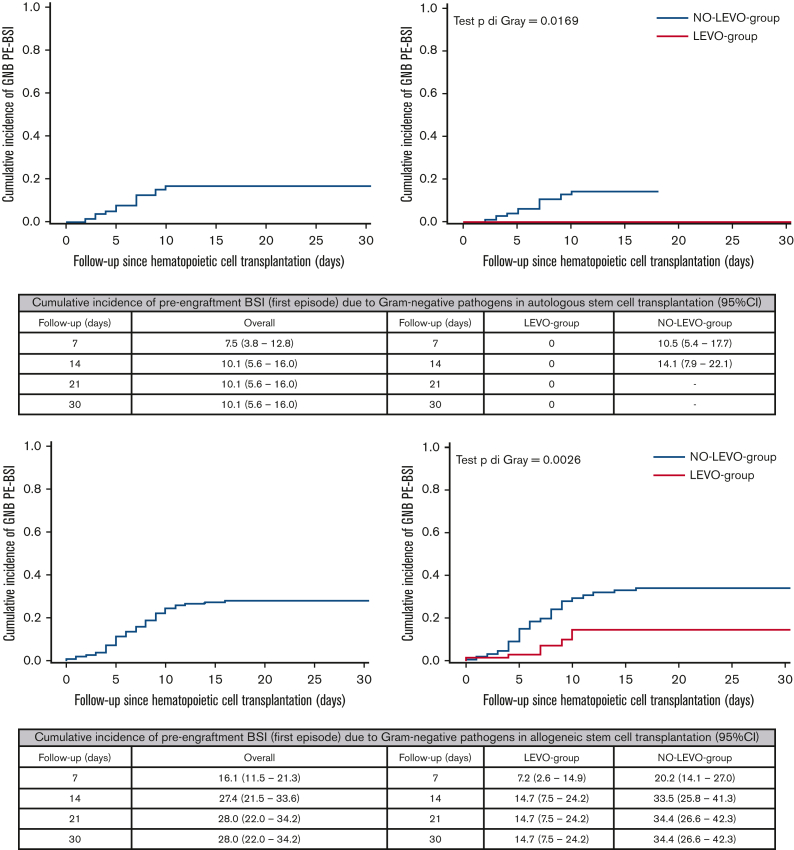
Fluoroquinolone prophylaxis's (FQ-P) usefulness in patients with neutropenia is controversial. In recent decades, Italian epidemiological data has shown worrisome rates of FQ resistance. A single-center cohort study on 136 autologous stem cell transplantations (ASCTs) and 223 allogeneic hematopoietic stem cell transplantations (allo-HSCTs) was performed from January 2018 to December 2020. Piperacillin/tazobactam was the first-line therapy for febrile neutropenia (FN). Since February 2019, FQ-P has been omitted. We evaluated the day +30 posttransplant cumulative incidence function (CIF) of gram-negative bacteria pre-engraftment bloodstream infections (PE-BSIs) and any changes in antimicrobial resistance, FN, and infection-related mortality (IRM). In ASCTs, ≥1 FN episode occurred in 74.3% of transplants, without differences among groups (P = .66). CIF of gram-negative bacteria PE-BSI was 10.1%, with a significant difference according to FQ-P (0% [LEVO-group] vs 14.1% [NO-LEVO-group], P = .016). CIF of IRM was 0% in both groups. In allo-HSCTs, ≥1 FN episode occurred in 96.4% of transplants, without differences among groups (P = .72). CIF of gram-negative bacteria PE-BSI was 28%, significantly higher without FQ-P (14.7% [LEVO-group] vs 34.4% [NO-LEVO-group], P = .003). CIF of IRM was 5%, superimposable in both groups (P = .62). Comparing antimicrobial resistance among gram-negative bacteria of allo-HSCT setting, in the group without FQ-P, a significantly higher proportion of pathogens was susceptible to piperacillin/tazobactam (71% vs 30%, P = .026), FQ (49% vs 10%, P = .03), and carbapenems (95% vs 50%, P = .001). FQ-P discontinuation increased gram-negative bacteria PE-BSI but did not impact IRM, both in the ASCT and allo-HSCT settings; importantly, it concurred to significantly decrease antimicrobial resistance in gram-negative bacteria.
氟喹诺酮类预防(FQ-P)在中性粒细胞减少症患者中的作用存在争议。近几十年来,意大利的流行病学数据显示,氟喹诺酮类耐药率令人担忧。一项针对 136 例自体干细胞移植(ASCT)和 223 例异基因造血干细胞移植(allo-HSCT)的单中心队列研究于 2018 年 1 月至 2020 年 12 月进行。哌拉西林/他唑巴坦是发热性中性粒细胞减少症(FN)的一线治疗药物。自 2019 年 2 月以来,已停止使用 FQ-P。我们评估了移植后第 30 天的革兰氏阴性菌定植前血流感染(PE-BSI)累积发生率(CIF)以及抗菌药物耐药性、FN 和感染相关死亡率(IRM)的任何变化。在 ASCT 中,74.3%的移植患者发生≥1 次 FN 发作,各组之间无差异(P=0.66)。革兰氏阴性菌 PE-BSI 的 CIF 为 10.1%,FQ-P 存在显著差异(0%[LEVO 组] vs. 14.1%[NO-LEVO 组],P=0.016)。两组的 IRM 的 CIF 均为 0%。在 allo-HSCT 中,96.4%的移植患者发生≥1 次 FN 发作,各组之间无差异(P=0.72)。革兰氏阴性菌 PE-BSI 的 CIF 为 28%,无 FQ-P 时显著升高(14.7%[LEVO 组] vs. 34.4%[NO-LEVO 组],P=0.003)。两组的 IRM 的 CIF 均为 5%,无差异(P=0.62)。比较 allo-HSCT 中革兰氏阴性菌的抗菌药物耐药性,无 FQ-P 组的病原体对哌拉西林/他唑巴坦(71% vs. 30%,P=0.026)、氟喹诺酮(49% vs. 10%,P=0.03)和碳青霉烯类(95% vs. 50%,P=0.001)的敏感性显著更高。ASCT 和 allo-HSCT 中,停止使用 FQ-P 增加了革兰氏阴性菌 PE-BSI,但并未影响 IRM;重要的是,它还显著降低了革兰氏阴性菌的抗菌药物耐药性。