Armour Richard, Learning Charmane, Trojanowski Jan
Ambulance Victoria; Monash University; Charles Sturt University.
British Columbia Emergency Health Services; Columbia Paramedic Academy.
Br Paramed J. 2022 Sep 1;7(2):38-42. doi: 10.29045/14784726.2022.09.7.2.38.
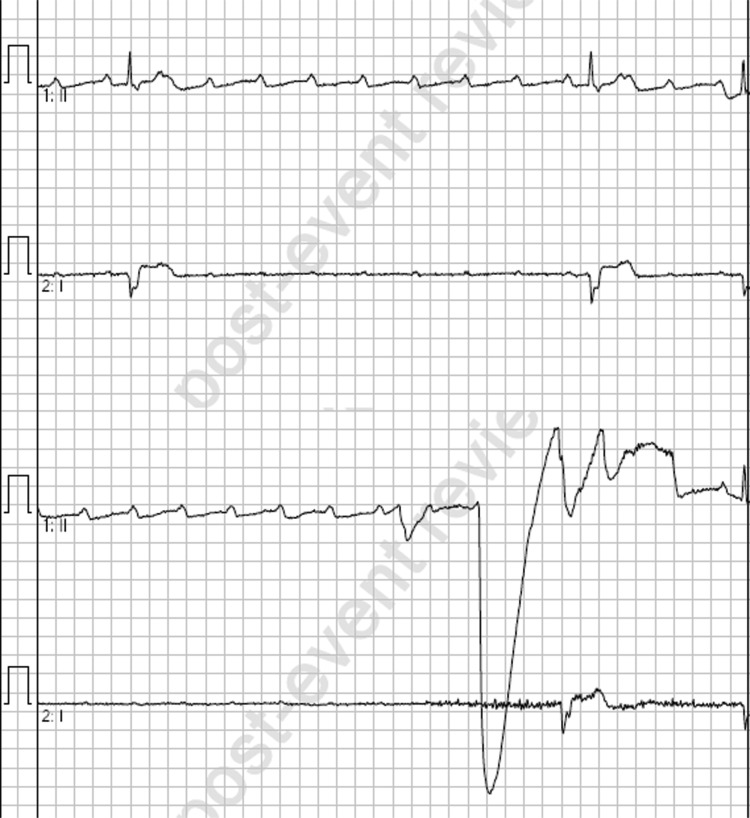
Bradyarrhythmias are a common entity in both emergency and out-of-hospital (OOH) medicine. In unstable bradycardic patients, paramedics will often initiate life-saving therapies in the OOH setting. Clinical guidelines for bradyarrhythmias are largely consistent across the globe, with intravenous (IV) atropine recommended as a first-line therapy, escalating to IV adrenaline or isoprenaline and transcutaneous pacing where atropine is unsuccessful. In this case report, we describe a case in the OOH setting of ventricular standstill following the administration of atropine to a patient with bradycardia and 2:1 heart block.
The patient was a 77-year-old female presenting with a symptomatic 2:1 heart block. Following a single dose of 600 micrograms IV atropine, the patient deteriorated into ventricular standstill with a loss of consciousness and decorticate posturing. The patient was successfully managed with an IV infusion of adrenaline and subsequently received an implanted pacemaker in hospital.
The paradoxical worsening of this patient's bradycardia following atropine administration may have been related to the location of the heart block. It has been shown that patients with atrioventricular blocks at the level of the His-Purkinje fibres (infranodal) are at an increased risk of adverse events following atropine administration, while those at the nodal level or secondary to increased vagal tone are more likely to respond favourably. Paramedics should be prepared to manage unexpected adverse events secondary to atropine administration in patients with heart block.
缓慢性心律失常在急诊医学和院外医疗中都很常见。对于不稳定的缓慢性心律失常患者,护理人员通常会在院外环境中启动挽救生命的治疗措施。全球范围内,缓慢性心律失常的临床指南基本一致,推荐静脉注射阿托品作为一线治疗药物,若阿托品治疗无效,则升级为静脉注射肾上腺素或异丙肾上腺素,并进行经皮起搏。在本病例报告中,我们描述了一例在院外环境中,对一名患有心动过缓和2:1房室传导阻滞的患者使用阿托品后发生心室停搏的病例。
患者为一名77岁女性,表现为有症状的2:1房室传导阻滞。静脉注射600微克阿托品单次剂量后,患者病情恶化,陷入心室停搏,意识丧失并出现去皮层姿势。患者通过静脉输注肾上腺素成功救治,随后在医院接受了植入式起搏器。
该患者使用阿托品后心动过缓反而加重,可能与房室传导阻滞的部位有关。研究表明,希氏束-浦肯野纤维水平(结下)的房室传导阻滞患者在使用阿托品后发生不良事件的风险增加,而结水平或继发于迷走神经张力增加的患者更可能有良好反应。护理人员应做好准备,应对心脏传导阻滞患者使用阿托品后出现的意外不良事件。