Department of Paediatric and Adult Rheumatology, Motol University Hospital, Prague, Czech Republic.
Department of Radiology, Second Faculty of Medicine, Charles University and Motol University Hospital, Prague, Czech Republic.
Pediatr Rheumatol Online J. 2022 Dec 1;20(1):108. doi: 10.1186/s12969-022-00772-w.
Chronic Recurrent Multifocal Osteomyelitis (CRMO) is an autoinflammatory bone disorder with predominantly paediatric onset. Children present with multifocal osteolytic lesions accompanied by bone pain and soft tissue swelling. Patients often exhibit extraosseous co-morbidities such as psoriasis, inflammatory bowel disease, and arthritis.
Comparison of children with two different phenotypes of CRMO defined by presence or absence of extraosseous co-morbidities.
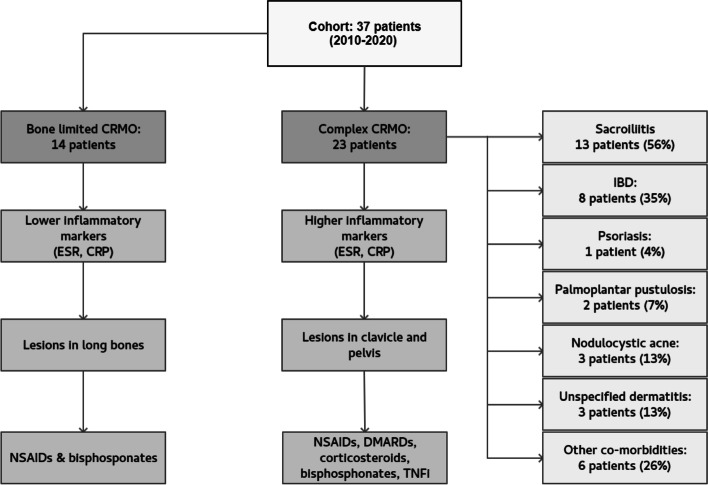
Children diagnosed with CRMO at the Motol University Hospital between 2010 and 2020 were retrospectively reviewed, and according to the absence or presence of extraosseous manifestations divided into two cohorts - bone limited CRMO and complex CRMO. The two groups were compared in terms of demographic data, age at disease onset, number and site of bone lesions, laboratory biomarker values, and need of escalation to a second-line therapy.
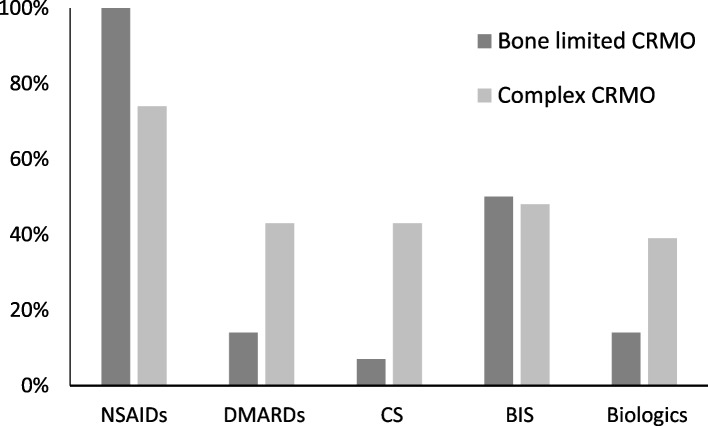
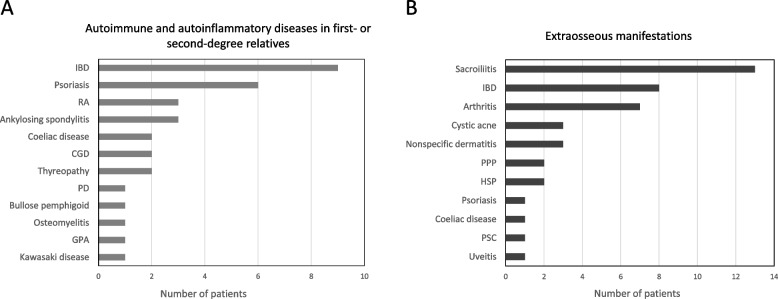
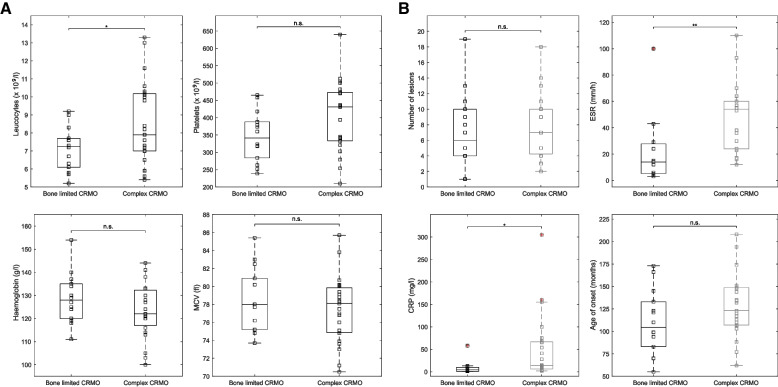
Thirty-seven children (30 female, 7 male) with confirmed CRMO were included in the analysis. The mean age at disease onset was 10 years. All but 3 patients presented with multifocal disease. Twenty-three children (62%) had at least one extraosseous manifestation (13 sacroiliitis, 8 inflammatory bowel disease, 6 skin disease [acne, pustulosis, or psoriasis], 7 arthritis). Complex CRMO was associated with a significantly higher ESR rate (p = 0.0064) and CRP level (p = 0.018). The groups did not differ in number of foci or in age at disease onset. Bone lesion distribution differed between the two groups with significantly more frequent involvement of clavicle (p = 0.011) and pelvis (p = 0.038) in patients with complex CRMO. Children with complex CRMO more often needed escalation of therapy to DMARDs and biologic agents.
Our data suggest that CRMO affecting solely the skeleton has milder course compared to complex CRMO with extraskeletal features. Further studies are needed to explore the clinical as well as the patient reported outcomes and promote individually tailored therapeutic strategies in both CRMO phenotypes.
慢性复发性多灶性骨髓炎(CRMO)是一种主要发生于儿童的自身炎症性骨病。儿童表现为多发性溶骨性病变,伴有骨痛和软组织肿胀。患者常伴有骨外合并症,如银屑病、炎症性肠病和关节炎。
比较两种不同表型的 CRMO 患儿,一种表现为有骨外合并症,另一种表现为无骨外合并症。
回顾性分析 2010 年至 2020 年在莫托夫大学医院诊断为 CRMO 的患儿,根据有无骨外表现将其分为两组 - 单纯型 CRMO 和复杂型 CRMO。比较两组患儿的人口统计学数据、发病年龄、骨病变部位和数量、实验室生物标志物值以及是否需要升级二线治疗。
37 例(30 名女性,7 名男性)CRMO 患儿纳入分析。发病年龄平均为 10 岁。除 3 例外,所有患儿均表现为多发病灶。23 例(62%)患儿至少有一个骨外表现(13 例骶髂关节炎、8 例炎症性肠病、6 例皮肤疾病[痤疮、脓疱病或银屑病]、7 例关节炎)。复杂型 CRMO 患儿的 ESR 率(p=0.0064)和 CRP 水平(p=0.018)显著更高。两组患儿的病灶数量和发病年龄无差异。两组患儿的骨病变分布不同,复杂型 CRMO 患儿的锁骨(p=0.011)和骨盆(p=0.038)受累频率显著更高。复杂型 CRMO 患儿更常需要升级为 DMARDs 和生物制剂治疗。
本研究数据表明,单纯累及骨骼的 CRMO 与伴有骨外表现的复杂型 CRMO 相比,其病程较轻。需要进一步研究以探讨两种 CRMO 表型的临床和患者报告结局,并促进个体化治疗策略的制定。