Department of Radiation Oncology, The Naef K. Basile Cancer Institute, The American University of Beirut Medical Center, Bliss Street, Riad El Solh, Beirut, 11072030, Lebanon.
Department of Radiation Oncology, King Hussein Cancer Center, Amman, Jordan.
BMC Urol. 2022 Dec 12;22(1):204. doi: 10.1186/s12894-022-01145-x.
A nadir Prostate-Specific Antigen (nPSA) of 0.06 ng/mL has been shown to be a strong independent predictor of biochemical recurrence-free survival (bRFS) in patients with intermediate or high-risk (HR) prostate cancer treated with definitive external beam radiation therapy (RT) and androgen deprivation therapy (ADT). We aimed to examine the association between the duration of ADT and bRFS in HR localized prostate cancer, based on nPSA.
Between 1998 and 2015, 204 patients with HR localized prostate cancer were identified. Of them, 157 patients (77.0%) reached the desired nPSA of < 0.06 ng/mL (favorable group), while 47 (23.0%) did not (unfavorable group). Duration of ADT varied among patients depending on physician preference, patient tolerance, and/or compliance. Survival outcomes were calculated using Kaplan-Meier methods and predictors of outcomes using multi-variable cox regression model.
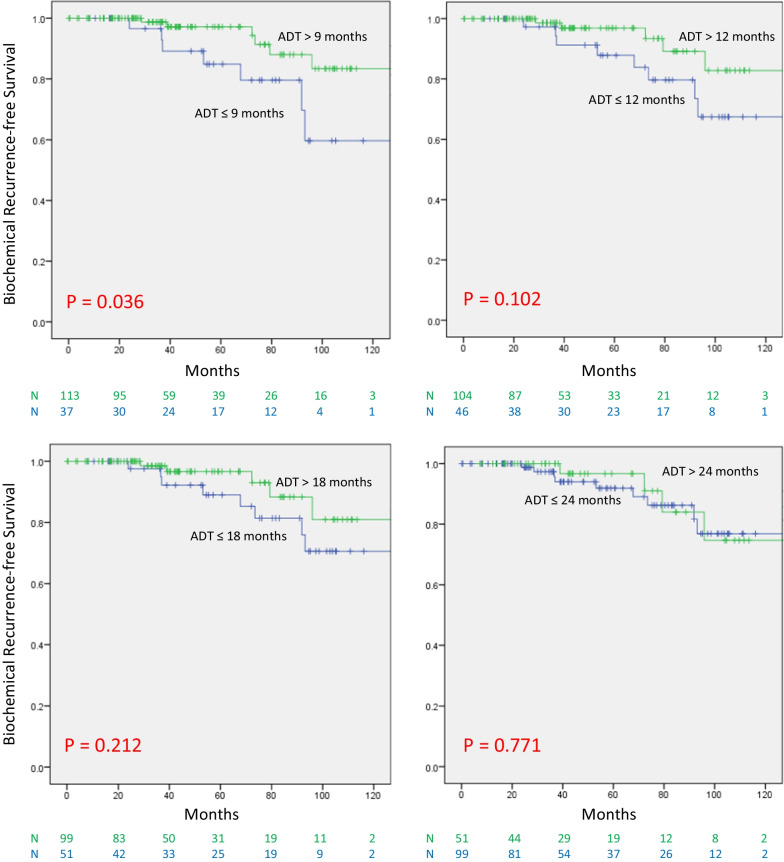
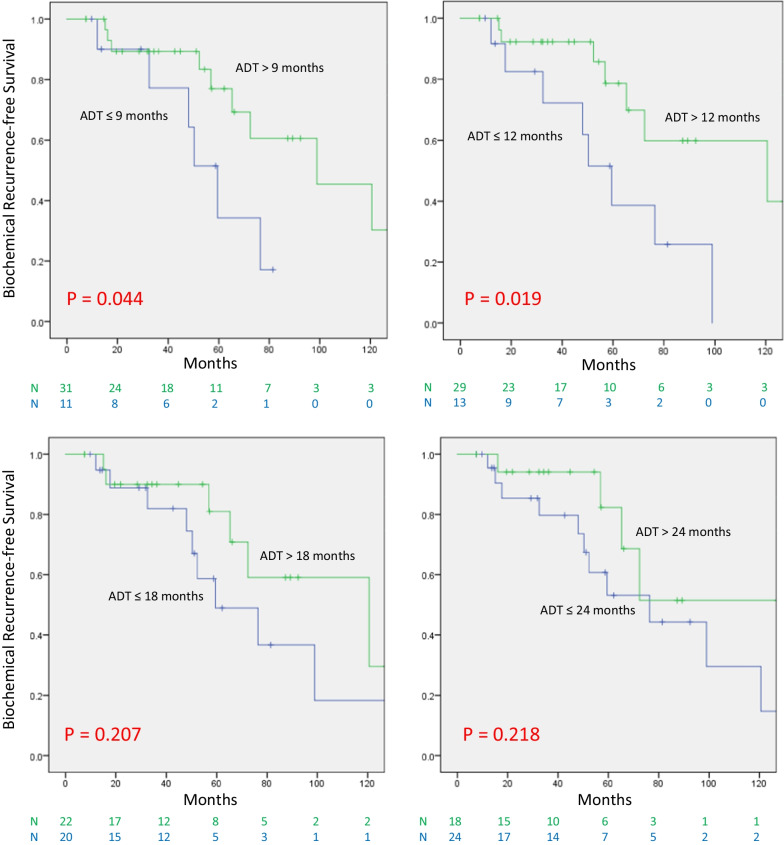
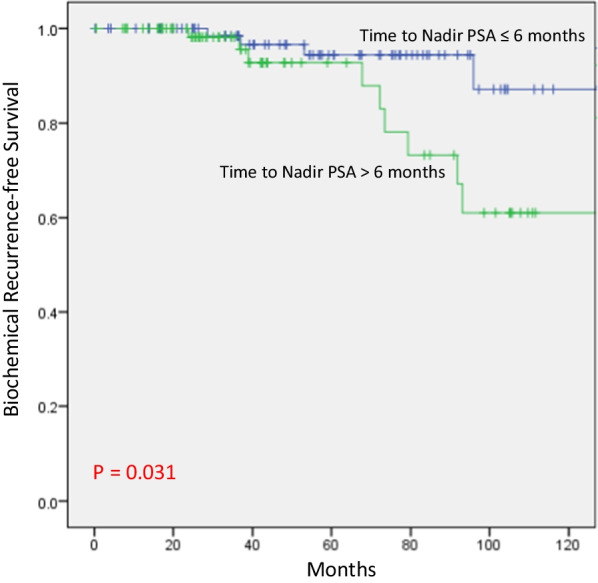
In the favorable group, ADT for at least 12 months lead to superior bRFS compared to ≤ 9 months of ADT (P = 0.036). However, no significant difference was seen when examining the value of receiving ADT beyond 12, 18, or 24 months, respectively. On univariate analysis for bRFS, the use of ADT for at least 12 months was significant (P = 0.012) as well as time to nadir PSA (tnPSA), (≤ 6 vs > 6 months); (P = 0.043). The presenting T stage was borderline significant (HR 3.074; 95% CI 0.972-9.719; P = 0.056), while PSA at presentation, Gleason Score and age were not. On multivariate analysis, the use of ADT for 12 months (P = 0.012) and tnPSA (P = 0.037) remained significant. In the unfavorable group, receiving ADT beyond 9 and 12 months was associated with improved bRFS (P = 0.044 and 0.019, respectively). However, beyond 18 months, there was no significant difference.
In HR localized prostate cancer patients treated with definitive RT and ADT, the total duration of ADT may be adjusted according to treatment response using nPSA. In patients reaching a nPSA below 0.06 ng/mL, a total of 12 months of ADT may be sufficient, while in those not reaching a nPSA below 0.06 ng/mL, a total duration of 18 months is required.
已证明,对于接受根治性外照射放疗(RT)和雄激素剥夺疗法(ADT)治疗的中高危(HR)前列腺癌患者,前列腺特异性抗原(PSA)最低点(nPSA)为 0.06ng/mL 是生化无复发生存(bRFS)的强有力独立预测因子。我们旨在根据 nPSA 研究 HR 局限性前列腺癌中 ADT 持续时间与 bRFS 之间的关系。
1998 年至 2015 年,共确定了 204 例 HR 局限性前列腺癌患者。其中,157 例(77.0%)达到了期望的 nPSA<0.06ng/mL(有利组),而 47 例(23.0%)未达到(不利组)。ADT 的持续时间因患者而异,取决于医生的偏好,患者的耐受性和/或依从性。使用 Kaplan-Meier 方法计算生存结果,并使用多变量 Cox 回归模型预测结果。
在有利组中,与 ADT 持续时间≤9 个月相比,ADT 至少 12 个月可导致 bRFS 更好(P=0.036)。然而,当分别检查接受 ADT 超过 12、18 或 24 个月的价值时,未见显着差异。在 bRFS 的单变量分析中,ADT 的使用时间至少为 12 个月(P=0.012)和 PSA 最低点时间(tnPSA)(≤6 与>6 个月)(P=0.043)均有意义。表现 T 分期具有边缘显着性(HR 3.074;95%CI 0.972-9.719;P=0.056),而 PSA 初诊时,Gleason 评分和年龄无显着性。多变量分析中,ADT 持续时间为 12 个月(P=0.012)和 tnPSA(P=0.037)仍然具有显着性。在不利组中,接受 ADT 超过 9 个月和 12 个月与 bRFS 改善相关(P=0.044 和 0.019)。但是,超过 18 个月后,没有显着差异。
在接受根治性 RT 和 ADT 治疗的 HR 局限性前列腺癌患者中,可根据 nPSA 的治疗反应调整 ADT 的总持续时间。对于达到 nPSA 低于 0.06ng/mL 的患者,ADT 总持续时间可能为 12 个月就足够了,而对于未达到 nPSA 低于 0.06ng/mL 的患者,则需要总持续时间为 18 个月。