Flessa Steffen
Department of Health Care Management, Faculty of Law and Economics, University of Greifswald, 17487 Greifswald, Germany.
Healthcare (Basel). 2022 Dec 19;10(12):2580. doi: 10.3390/healthcare10122580.
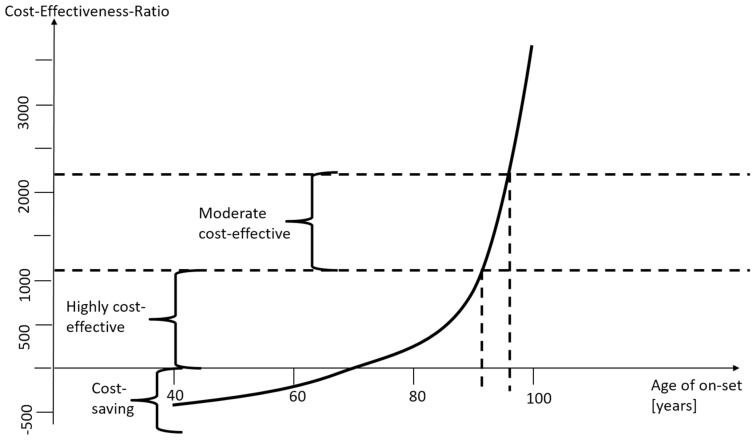
Cataract is a major cause of blindness worldwide. In particular, in low-income countries, the burden of disease as well as its direct and indirect economic cost are a major challenge for the population and economy. In many cases, it would be possible to prevent or cure blindness with a comparably simple cataract surgery, but many countries lack the resources to strengthen healthcare systems and implement broad cataract surgery programs reaching, in particular, the rural poor. In this paper, we analyse whether such an intervention could be cost-effective or even cost-saving for the respective health systems. We calculate the net value of the lifelong costs of cataract with and without surgery. This calculation includes direct costs (e.g., treatment, glasses, surgery) as well as indirect cost of the caregiver and the patient. We total all costs from the year of onset of cataract until death and discount the respective values to the year of onset. We define the surgery as cost-saving if the net-value of costs with surgery is lower than without surgery. If the cost per quality adjusted life year is lower than one gross national product per capita, we define the intervention as highly cost-effective. We find that the cost-effectiveness of cataract surgery depends on the age of onset of the disease and the age of surgery. If the surgery is performed with the beginning of severe impairment, even surgery of a 78-year-old patient is still cost-saving. Almost all possible constellations are highly cost-effective, only for the very old it is questionable whether the surgery should be performed. The simulations show that cataract surgery is one of the most cost-effective interventions. However, millions of people in low-income countries still have no chance to prevent or cure blindness due to limited resources. The findings of this paper clearly call for a stronger effort to reach poor and rural populations with this cost-effective service.
白内障是全球失明的主要原因。特别是在低收入国家,疾病负担及其直接和间接经济成本对人口和经济构成了重大挑战。在许多情况下,通过相对简单的白内障手术就有可能预防或治愈失明,但许多国家缺乏资源来加强医疗保健系统并实施广泛的白内障手术项目,尤其是覆盖农村贫困人口。在本文中,我们分析了这种干预措施对各自的卫生系统是否具有成本效益甚至是否能节省成本。我们计算了白内障患者手术和不手术情况下终身成本的净值。这种计算包括直接成本(如治疗、眼镜、手术)以及护理人员和患者的间接成本。我们汇总了从白内障发病年份到死亡的所有成本,并将各自的值折现到发病年份。如果手术情况下的成本净值低于不手术的情况,我们将手术定义为节省成本。如果每质量调整生命年的成本低于人均国民生产总值,我们将该干预措施定义为具有高度成本效益。我们发现白内障手术的成本效益取决于疾病的发病年龄和手术年龄。如果在严重视力损害开始时进行手术,即使是78岁患者的手术仍然是节省成本的。几乎所有可能的情况都具有高度成本效益,只有对于非常年老的患者,是否进行手术存在疑问。模拟结果表明,白内障手术是最具成本效益的干预措施之一。然而,由于资源有限,低收入国家仍有数百万人没有机会预防或治愈失明。本文的研究结果明确呼吁做出更大努力,为贫困和农村人口提供这种具有成本效益的服务。