De Geer Lina, Fredrikson Mats, Chew Michelle S
Department of Anaesthesiology and Intensive Care, and Department of Biomedical and Clinical Sciences, Linköping University, 581 83, Linköping, Sweden.
Division of Occupational and Environmental Medicine, Department of Clinical and Experimental Medicine and Forum Östergötland, All at Linköping University, 581 83, Linköping, Sweden.
Ann Intensive Care. 2022 Dec 31;12(1):120. doi: 10.1186/s13613-022-01098-2.
While frailty is a known predictor of adverse outcomes in older patients, its effect in younger populations is unknown. This prospective observational study was conducted in a tertiary-level mixed ICU to assess the impact of frailty on long-term survival in intensive care patients of different ages.
Data on premorbid frailty (Clinical Frailty Score; CFS), severity of illness (the Simplified Acute Physiology Score, third version; SAPS3), limitations of care and outcome were collected in 817 adult ICU patients. Hazard ratios (HR) for death within 180 days after ICU admission were calculated. Unadjusted and adjusted analyses were used to evaluate the association of frailty with outcome in different age groups.
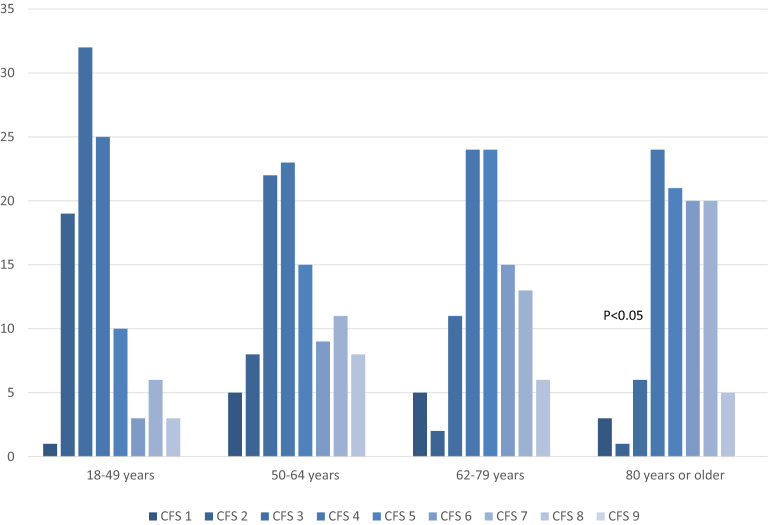
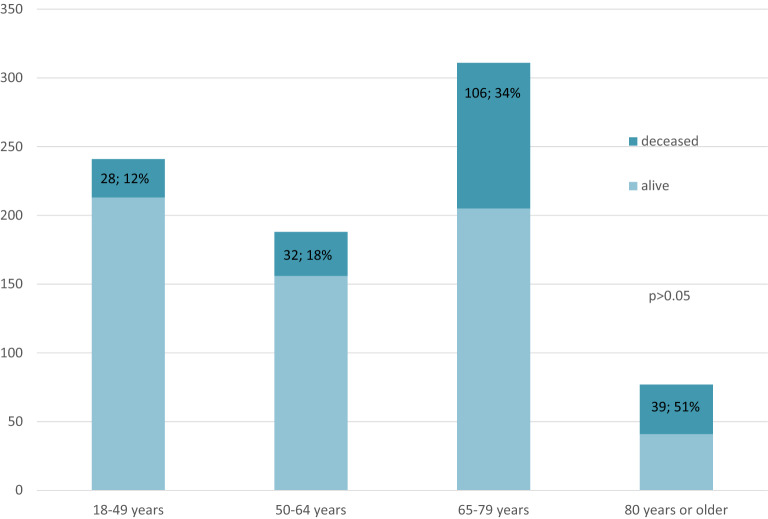
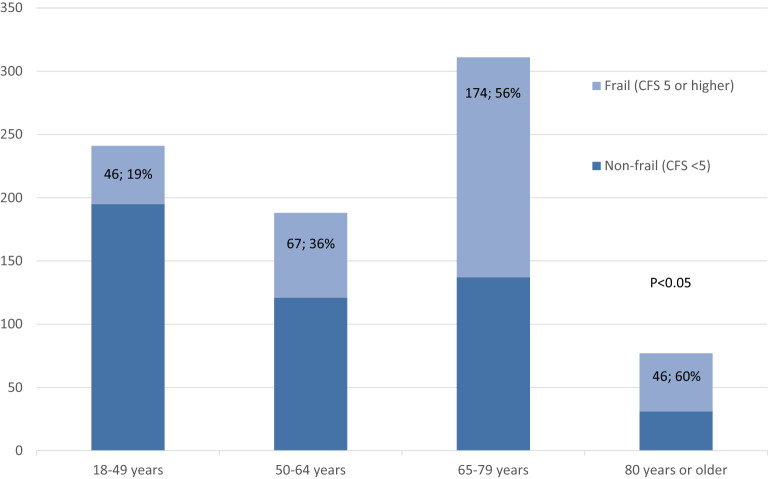
Patients were classified into predefined age groups (18-49 years (n = 241), 50-64 (n = 188), 65-79 (n = 311) and 80 years or older (n = 77)). The proportion of frail (CFS ≥ 5) patients was 41% (n = 333) in the overall population and increased with each age strata (n = 46 (19%) vs. n = 67 (36%) vs. n = 174 (56%) vs. n = 46 (60%), P < 0.05). Frail patients had higher SAPS3, more treatment restrictions and higher ICU mortality. Frailty was associated with an increased risk of 180-day mortality in all age groups (HR 5.7 (95% CI 2.8-11.4), P < 0.05; 8.0 (4.0-16.2), P < 0.05; 4.1 (2.2-6.6), P < 0.05; 2.4 (1.1-5.0), P = 0.02). The effect remained significant after adjustment for SAPS3, comorbidity and limitations of treatment only in patients aged 50-64 (2.1 (1.1-3.1), P < 0.05).
Premorbid frailty is common in ICU patients of all ages and was found in 55% of patients aged under 64 years. Frailty was independently associated with mortality only among middle-aged patients, where the risk of death was increased twofold. Our study supports the use of frailty assessment in identifying younger ICU patients at a higher risk of death.
虽然衰弱是老年患者不良预后的已知预测因素,但其在年轻人群中的影响尚不清楚。本前瞻性观察性研究在三级综合重症监护病房进行,以评估衰弱对不同年龄重症监护患者长期生存的影响。
收集了817例成年重症监护病房患者的病前衰弱数据(临床衰弱评分;CFS)、疾病严重程度(简化急性生理学评分第三版;SAPS3)、护理限制和预后情况。计算了重症监护病房入院后180天内死亡的风险比(HR)。采用未调整和调整分析来评估不同年龄组中衰弱与预后的关联。
患者被分为预定义的年龄组(18 - 49岁(n = 241)、50 - 64岁(n = 188)、65 - 79岁(n = 311)和80岁及以上(n = 77))。总体人群中衰弱(CFS≥5)患者的比例为41%(n = 333),且随每个年龄层增加(n = 46(19%)对n = 67(36%)对n = 174(56%)对n = 46(60%),P < 0.05)。衰弱患者的SAPS3更高,治疗限制更多,重症监护病房死亡率更高。衰弱与所有年龄组180天死亡率风险增加相关(HR 5.7(95%CI 2.8 - 11.4),P < 0.05;8.0(4.0 - 16.2),P < 0.05;4.1(2.2 - 6.6),P < 0.05;2.4(1.1 - 5.0),P = 0.02)。仅在50 - 64岁患者中,调整SAPS3合并症和治疗限制后,该效应仍显著(2.1(1.1 - 3.1),P <