Yu Zhenwei, Liu Xiaofen, Du Xiaoxing, Chen Huiying, Zhao Feng, Zhou Zhihui, Wang Yu, Zheng Yang, Bergen Phillip J, Li Xi, Sun Renhua, Fang Li, Li Wanzhen, Fan Yaxin, Wu Hailan, Guo Beining, Li Jian, Yu Yunsong, Zhang Jing
Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, China.
Institute of Antibiotics, Huashan Hospital, Fudan University, Shanghai, China.
Front Pharmacol. 2022 Dec 16;13:975066. doi: 10.3389/fphar.2022.975066. eCollection 2022.
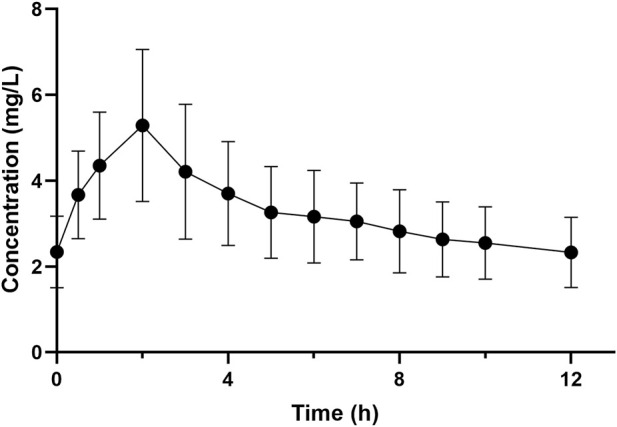
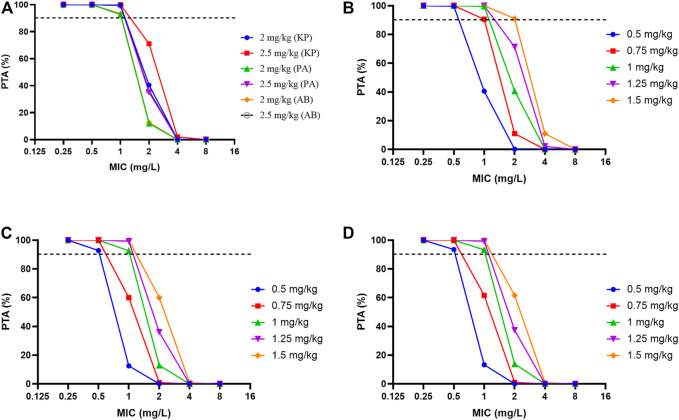
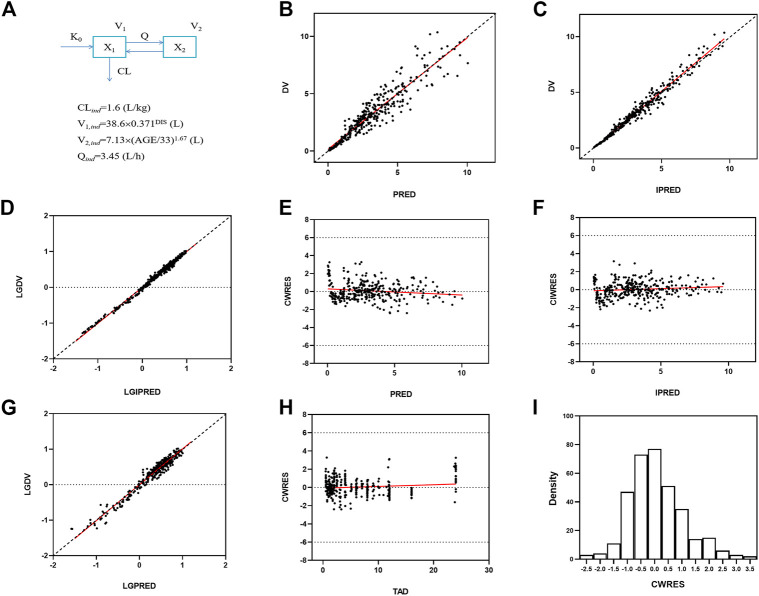
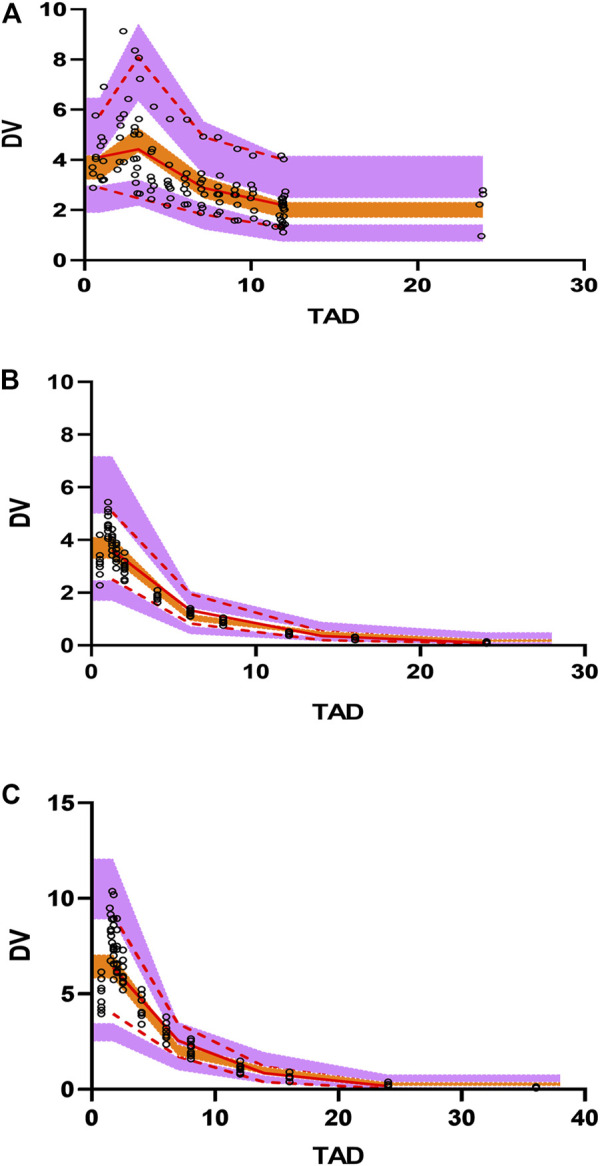
Polymyxin B is a last-line therapy for carbapenem-resistant microorganisms. However, a lack of clinical pharmacokinetic/pharmacodynamic (PK/PD) data has substantially hindered dose optimization and breakpoint setting. A prospective, multi-center clinical trial was undertaken with polymyxin B [2.5 mg/kg loading dose (3-h infusion), 1.25 mg/kg/12 h maintenance dose (2-h infusion)] for treatment of carbapenem-resistant (CRKP) bloodstream infections (BSI). Safety, clinical and microbiological efficacy were evaluated. A validated liquid chromatography-tandem mass spectrometry (LC-MS/MS) method was applied to determine the concentrations of polymyxin B in blood samples. Population pharmacokinetic (PK) modeling and Monte Carlo simulations were conducted to examine the susceptibility breakpoint for polymyxin B against BSI caused by CRKP. Nine patients were enrolled and evaluated for safety. Neurotoxicity (5/9), nephrotoxicity (5/9), and hyperpigmentation (1/9) were recorded. Blood cultures were negative within 3 days of commencing therapy in all 8 patients evaluated for microbiological efficacy, and clinical cure or improvement occurred in 6 of 8 patients. C and C following the loading dose were 5.53 ± 1.80 and 1.62 ± 0.41 mg/L, respectively. With maintenance dosing, AUC was 79.6 ± 25.0 mg h/L and C 3.35 ± 1.06 mg/L. Monte Carlo simulations indicated that a 1 mg/kg/12-hourly maintenance dose could achieve >90% probability of target attainment (PTA) for isolates with minimum inhibitory concentration (MIC) ≤1 mg/L. PTA dropped substantially for MICs ≥2 mg/L, even with a maximally recommended daily dose of 1.5 mg/kg/12-hourly. This is the first clinical PK/PD study evaluating polymyxin B for BSI. These results will assist to optimize polymyxin B therapy and establish its breakpoints for CRKP BSI.
多粘菌素B是治疗对碳青霉烯类耐药微生物的最后一线疗法。然而,临床药代动力学/药效学(PK/PD)数据的缺乏严重阻碍了剂量优化和折点设定。开展了一项前瞻性多中心临床试验,使用多粘菌素B[2.5mg/kg负荷剂量(3小时输注),1.25mg/kg/12小时维持剂量(2小时输注)]治疗耐碳青霉烯类肺炎克雷伯菌(CRKP)血流感染(BSI)。评估了安全性、临床和微生物学疗效。应用经过验证的液相色谱-串联质谱(LC-MS/MS)方法测定血样中多粘菌素B的浓度。进行群体药代动力学(PK)建模和蒙特卡洛模拟,以研究多粘菌素B对CRKP引起的BSI的药敏折点。招募了9名患者并评估其安全性。记录到神经毒性(5/9)、肾毒性(5/9)和色素沉着过度(1/9)。在评估微生物学疗效的所有8名患者中,开始治疗后3天内血培养均为阴性,8名患者中有6名实现了临床治愈或改善。负荷剂量后的Cmax和Cmin分别为5.53±1.80和1.62±0.41mg/L。维持给药时,AUC为79.6±25.0mg·h/L,Cmin为3.35±1.06mg/L。蒙特卡洛模拟表明,对于最低抑菌浓度(MIC)≤1mg/L的分离株,1mg/kg/12小时的维持剂量可实现>90%的目标达成概率(PTA)。即使最大推荐日剂量为1.5mg/kg/12小时,对于MIC≥2mg/L的情况,PTA也会大幅下降。这是第一项评估多粘菌素B治疗BSI的临床PK/PD研究。这些结果将有助于优化多粘菌素B治疗,并为CRKP BSI确定其折点。