Petersen Harrington Shariska, Balmaceda Julia, Spoozak Lori, Jewell Andrea, Fitzgerald-Wolff Sharon
Division of Gynecologic Oncology, Department of Obstetrics & Gynecology, University of Kansas Medical Center, Kansas City, KS, United States.
University of Kansas School of Medicine, University of Kansas Medical Center, Kansas City, KS, United States.
Gynecol Oncol Rep. 2022 Dec 13;44:101123. doi: 10.1016/j.gore.2022.101123. eCollection 2022 Dec.
Endometrial cancer is often directly related to obesity and interventions for weight loss have mixed results. Risk factors for continued weight gain after diagnosis are not clearly defined in the literature. The objective of this study is to describe risk factors associated with increased body mass index (BMI) trajectory among endometrial cancer patients.
Patients who were surgically treated for endometrial cancer at a single institution between 2010 and 2015 were identified. Demographics including age, race/ethnicity and estimated median income at diagnosis were obtained. BMI at five time points after diagnosis were calculated. BMI trajectories were estimated by latent class growth modeling using the PROC TRAJ procedure in SAS. Chi-squared tests and ANOVA were used to assess differences between trajectory groups. Statistical significance was set to a p-value < 0.05.
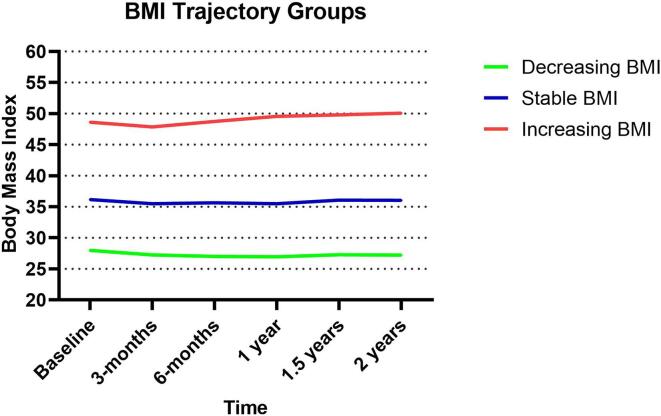
Of 695 patients included in the study, the average age at diagnosis was 62 years and over 70% of patients were obese at baseline. Patients experienced increasing, stable, or decreasing BMI over 2 years following diagnosis. Patients with younger age and lower estimated median income were most likely to be in the increasing BMI group. Among obese patients, those with Class I obesity (BMI 30 to 34.9 kg/m) were most likely to experience decreasing BMI and those with Class III obesity (BMI > 40 kg/m) were most likely to experience increasing BMI, p < 0.0001.
A third of endometrial cancer survivors experience increasing BMI. Severity of obesity at diagnosis matters, patients with severe obesity (Class III) were most likely to experience weight gain.
子宫内膜癌通常与肥胖直接相关,而减肥干预的效果参差不齐。文献中尚未明确诊断后体重持续增加的风险因素。本研究的目的是描述子宫内膜癌患者体重指数(BMI)轨迹增加相关的风险因素。
确定2010年至2015年期间在单一机构接受子宫内膜癌手术治疗的患者。获取包括年龄、种族/民族以及诊断时估计的收入中位数等人口统计学数据。计算诊断后五个时间点的BMI。使用SAS中的PROC TRAJ程序通过潜在类别增长模型估计BMI轨迹。采用卡方检验和方差分析来评估轨迹组之间的差异。统计学显著性设定为p值<0.05。
在纳入研究的695名患者中,诊断时的平均年龄为62岁,超过70%的患者在基线时肥胖。患者在诊断后的两年内BMI呈现上升、稳定或下降趋势。年龄较小且估计收入中位数较低的患者最有可能属于BMI上升组。在肥胖患者中,I类肥胖(BMI 30至34.9 kg/m)的患者最有可能BMI下降,而III类肥胖(BMI>40 kg/m)的患者最有可能BMI上升,p<0.0001。
三分之一的子宫内膜癌幸存者BMI上升。诊断时肥胖的严重程度很重要,重度肥胖(III类)患者最有可能体重增加。