Department of Pediatrics, Endocrinology, Diabetology and Nephrology, Maria Konopnicka University Pediatrics Center, Lodz, Poland.
Department of Pediatrics, Diabetology, Endocrinology and Nephrology, Medical University of Lodz, Lodz, Poland.
Front Endocrinol (Lausanne). 2022 Dec 14;13:1061671. doi: 10.3389/fendo.2022.1061671. eCollection 2022.
One of the most important complications of obesity is insulin resistance, which leads to carbohydrate metabolism disorders such as type 2 diabetes. However, obesity is also associated with development of an autoimmune response against various organs, including pancreatic beta cells. The prevalence of such autoimmune processes in children and their possible contribution to the increased incidence of type 1 diabetes is currently unclear. Therefore, the present study assessed the prevalence of autoantibodies against pancreatic islet beta cell's antigens in children and adolescents with simple obesity.
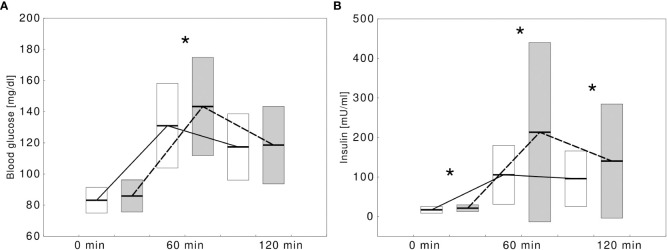
This prospective observational study included pediatric patients (up to 18 years of age) with simple obesity hospitalized between 2011 and 2016 at the Department of Pediatrics, Diabetology, Endocrinology and Nephrology of the Medical University of Lodz. Children with acute or chronic conditions that might additionally affect insulin resistance or glucose metabolism were excluded. Collected clinical data included sex, age, sexual maturity ratings (Tanners scale), body height and weight, waist and hip circumference, amount of body fat and lean body mass. Each participant underwent a 2-hour oral glucose tolerance test with simultaneous measurements of glycaemia and insulinemia at 0, 60 and 120. In addition, glycated hemoglobin HbA1c, fasting and stimulated c-peptide, total cholesterol, as well as high- and low-density cholesterol and triglycerides were measured. Insulin resistance was assessed by calculating HOMA-IR index. The following autoantibodies against pancreatic islet beta cells were determined in each child: ICA - antibodies against cytoplasmic antigens of pancreatic islets, GAD - antibodies against glutamic acid decarboxylase, ZnT8 - antibodies against zinc transporter, IA2 - antibodies against tyrosine phosphatase, IAA - antibodies against insulin.
The study group included 161 children (57.4% boys, mean age 13.1 ± 2.9 years) with simple obesity (mean BMI z-score +2.2 ± 1.6). Among them, 28 (17.4%) were diagnosed with impaired glucose metabolism during OGTT [23 (82.2%) - isolated impaired glucose tolerance (IGT), 3 (10.7%) - isolated impaired fasting glucose (IFG), 2 (7.1%) - IFG and IGT]. Of the children tested, 28 (17.4%) were tested positive for at least one islet-specific autoantibody [with similar percentages in boys (15, 17.4%) and girls (13, 17.3%), p=0.9855], with ICA being the most common (positive in 18, 11.2%), followed by IAA (7, 4.3%), ZnT8 (5, 3.1%), GADA (3, 1.9%) and IA2 (1, 0.6%). There was no association between the presence of the tested antibodies and age, sex, stage of puberty, parameters assessing the degree of obesity, HbA1c, lipid levels and basal metabolic rate. However, autoantibody-positive subjects were more likely to present IFG or IGT in OGTT compared to those who tested completely negative (9, 32.1% vs 19, 14.3%, p=0.0280). Their HOMA-IR was also significantly higher (HOMA-IR: 4.3 ± 1.9 vs 3.4 ± 1.9, p=0.0203) and this difference remained statistically significant after adjusting for sex and age (p=0.0340).
Children and adolescents with simple obesity presented a higher prevalence of markers of autoimmune response against pancreatic beta cells than the general population. Most often, they had only one type of antibody - ICA. The presence of autoimmune response indicators against pancreatic islet antigens is more common in obese patients with impaired carbohydrate metabolism and is associated with lower insulin sensitivity.
肥胖症最重要的并发症之一是胰岛素抵抗,这会导致 2 型糖尿病等碳水化合物代谢紊乱。然而,肥胖症也与各种器官的自身免疫反应的发展有关,包括胰岛β细胞。目前尚不清楚此类自身免疫过程在儿童中的流行程度及其对 1 型糖尿病发病率增加的可能贡献。因此,本研究评估了单纯性肥胖儿童和青少年胰岛β细胞抗原自身抗体的流行情况。
这是一项前瞻性观察性研究,纳入了 2011 年至 2016 年期间在罗兹医科大学儿科、糖尿病学、内分泌学和肾病科住院的单纯性肥胖的儿科患者(年龄不超过 18 岁)。排除有急性或慢性疾病可能另外影响胰岛素抵抗或葡萄糖代谢的患者。收集的临床数据包括性别、年龄、性成熟评分(Tanner 量表)、身高和体重、腰围和臀围、体脂肪量和瘦体重。每位患者均进行了 2 小时口服葡萄糖耐量试验,同时在 0'、60'和 120'时测量血糖和胰岛素。此外,还测量了糖化血红蛋白 HbA1c、空腹和刺激 C 肽、总胆固醇以及高低密度胆固醇和甘油三酯。通过计算 HOMA-IR 指数评估胰岛素抵抗。在每个孩子中均测定了以下胰岛β细胞自身抗体:ICA - 胰岛细胞质抗原抗体、GAD - 谷氨酸脱羧酶抗体、ZnT8 - 锌转运体抗体、IA2 - 酪氨酸磷酸酶抗体、IAA - 胰岛素抗体。
研究组包括 161 名儿童(57.4%为男性,平均年龄 13.1 ± 2.9 岁)患有单纯性肥胖症(平均 BMI z 评分+2.2 ± 1.6)。其中,28 名(17.4%)在 OGTT 期间被诊断为葡萄糖代谢受损[23 名(82.2%)为孤立性糖耐量受损(IGT),3 名(10.7%)为孤立性空腹血糖受损(IFG),2 名(7.1%)为 IFG 和 IGT]。在接受检测的儿童中,28 名(17.4%)至少有一种胰岛特异性自身抗体呈阳性[男孩(15 名,17.4%)和女孩(13 名,17.3%)的百分比相似,p=0.9855],ICA 最为常见(阳性 18 例,11.2%),其次是 IAA(7 例,4.3%)、ZnT8(5 例,3.1%)、GADA(3 例,1.9%)和 IA2(1 例,0.6%)。在存在检测到的抗体与年龄、性别、青春期阶段、肥胖程度评估参数、HbA1c、血脂水平和基础代谢率之间没有关联。然而,与完全阴性的受试者相比,自身抗体阳性的受试者在 OGTT 中更有可能出现 IFG 或 IGT(9 名,32.1% vs 19 名,14.3%,p=0.0280)。他们的 HOMA-IR 也显著更高(HOMA-IR:4.3 ± 1.9 vs 3.4 ± 1.9,p=0.0203),并且在调整性别和年龄后这一差异仍然具有统计学意义(p=0.0340)。
单纯性肥胖的儿童和青少年表现出比一般人群更高的胰岛β细胞自身免疫反应标志物的流行率。他们最常见的是只有一种抗体 - ICA。在碳水化合物代谢受损的肥胖患者中,胰岛抗原自身免疫反应标志物的存在更为常见,并且与较低的胰岛素敏感性相关。