Division of Prenatal Medicine, Fetal Surgery and Gynecological Ultrasound, Department of Obstetrics and Gynecology, University Hospital Cologne and Faculty of Medicine, University of Cologne, Cologne, Germany.
Department of Neonatology, University Hospital of Cologne, Cologne, Germany.
Arch Gynecol Obstet. 2024 Jan;309(1):145-158. doi: 10.1007/s00404-022-06905-6. Epub 2023 Jan 5.
To assess the spectrum of underlying pathologies, the intrauterine course and postnatal outcome of 46 fetuses with megacystis that underwent intrauterine vesico-amniotic shunting (VAS) with the Somatex® shunt in a single center.
Retrospective analysis of 46 fetuses with megacystis that underwent VAS either up to 14 + 0 weeks (early VAS), between 14 + 1 and 17 + 0 weeks (intermediate VAS) or after 17 + 0 weeks of gestation (late VAS) in a single tertiary referral center. Intrauterine course, underlying pathology and postnatal outcome were assessed and correlated with the underlying pathology and gestational age at first VAS.
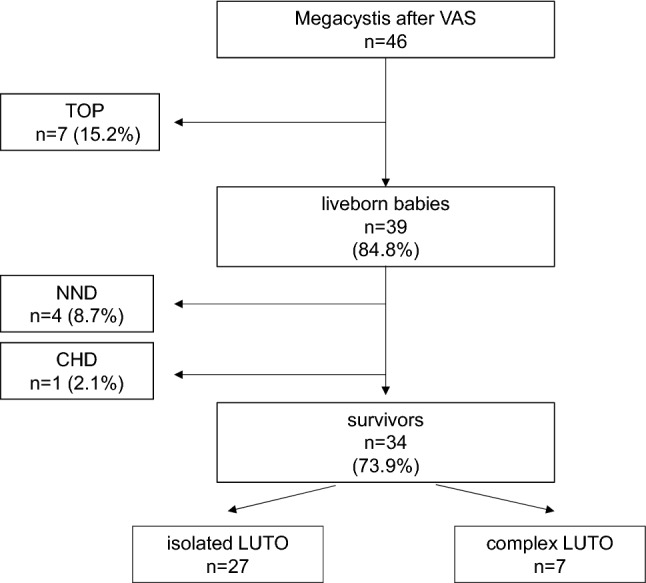
46 fetuses underwent VAS, 41 (89%) were male and 5 (11%) were female. 28 (61%) fetuses had isolated and 18 (39%) had complex megacystis with either aneuploidy (n = 1), anorectal malformations (n = 6), cloacal malformations (n = 3), congenital anomalies overlapping with VACTER association (n = 6) or Megacystis-Microcolon Intestinal-Hypoperistalsis Syndrome (MMIHS) (n = 2). The sonographic 'keyhole sign' significantly predicted isolated megacystis (p < 0.001). 7 pregnancies were terminated, 4 babies died in the neonatal period, 1 baby died at the age of 2.5 months and 34 (74%) infants survived until last follow-up. After exclusion of the terminated pregnancies, intention-to-treat survival rate was 87%. Mean follow-up period was 24 months (range 1-72). The underlying pathology was highly variable and included posterior urethral valve (46%), hypoplastic or atretic urethra (35%), MMIHS or prune belly syndrome (10%) and primary vesico-ureteral reflux (2%). In 7% no pathology could be detected postnatally. No sonographic marker was identified to predict the underlying pathology prenatally. 14 fetuses underwent early, 24 intermediate and 8 late VAS. In the early VAS subgroup, amnion infusion prior to VAS was significantly less often necessary (7%), shunt complications were significantly less common (29%) and immediate kidney replacement therapy postnatally became less often necessary (0%). In contrast, preterm delivery ≤ 32 + 0 weeks was more common (30%) and survival rate was lower (70%) after early VAS compared to intermediate or late VAS. Overall, 90% of liveborn babies had sufficient kidney function without need for kidney replacement therapy until last follow-up, and 95% had sufficient pulmonary function without need for mechanical respiratory support. 18% of babies with complex megacystis suffered from additional health restrictions due to their major concomitant malformations.
Our data suggest that VAS is feasible from the first trimester onward. Early intervention has the potential to preserve neonatal kidney function in the majority of cases and enables neonatal survival in up to 87% of cases. Despite successful fetal intervention, parents should be aware of the potential of mid- or long-term kidney failure and of additional health impairments due to concomitant extra-renal anomalies that cannot be excluded at time of intervention.
评估在单一中心接受 Somatex®分流器行宫内囊腔-羊膜分流术(VAS)的 46 例巨膀胱胎儿的潜在病理学谱、宫内病程和产后结局。
回顾性分析在单一三级转诊中心接受 VAS 的 46 例巨膀胱胎儿的资料,VAS 时间分别为 14+0 周之前(早期 VAS)、14+1 周至 17+0 周之间(中期 VAS)或 17+0 周之后(晚期 VAS)。评估了宫内病程、潜在病理学和产后结局,并与首次 VAS 时的潜在病理学和孕龄相关。
46 例胎儿接受了 VAS,41 例(89%)为男性,5 例(11%)为女性。28 例(61%)胎儿为单纯性巨膀胱,18 例(39%)为复杂性巨膀胱,伴非整倍体(n=1)、肛门直肠畸形(n=6)、泄殖腔畸形(n=3)、与 VACTER 协会重叠的先天性异常(n=6)或巨膀胱-小结肠-肠蠕动不良综合征(MMIHS)(n=2)。超声“钥匙孔征”显著预测单纯性巨膀胱(p<0.001)。7 例妊娠终止,4 例新生儿死亡,1 例 2.5 月龄死亡,34 例(74%)婴儿存活至最后一次随访。排除终止妊娠后,意向治疗存活率为 87%。平均随访时间为 24 个月(范围 1-72)。潜在病理学高度多样化,包括后尿道瓣膜(46%)、发育不良或闭锁尿道(35%)、MMIHS 或梅干腹综合征(10%)和原发性膀胱输尿管反流(2%)。7%的病例在产后无法检测到病理学。产前没有发现可以预测潜在病理学的超声标志物。14 例胎儿接受了早期、24 例中期和 8 例晚期 VAS。在早期 VAS 亚组中,VAS 前羊膜内输注明显较少(7%),分流器并发症明显较少(29%),产后立即进行肾脏替代治疗的必要性明显降低(0%)。相反,早期 VAS 组早产儿(<32+0 周)更常见(30%),存活率较低(70%),而中期或晚期 VAS 组存活率为 90%。总体而言,90%的活产儿在最后一次随访前无需肾脏替代治疗即可获得足够的肾功能,95%的活产儿无需机械呼吸支持即可获得足够的肺功能。18%的复杂性巨膀胱患儿由于主要伴发的严重畸形而受到额外的健康限制。
我们的数据表明,VAS 从妊娠早期开始就是可行的。早期干预有可能在大多数情况下保留新生儿的肾功能,并使多达 87%的病例能够存活。尽管胎儿干预成功,但父母应意识到潜在的中期或长期肾功能衰竭和因无法在干预时排除的伴发肾外异常而导致的额外健康损害的可能性。