The Norwegian Air Ambulance Foundation, Research and Development, Oslo, Norway.
Institute of Basic Medical Sciences, University of Oslo, Oslo, Norway.
Scand J Trauma Resusc Emerg Med. 2023 Jan 5;31(1):1. doi: 10.1186/s13049-022-01065-7.
Rapid identification and treatment of stroke is crucial for the outcome of the patient. We aimed to determine the performance of glial fibrillary acidic protein (GFAP) independently and in combination with the Prehospital Stroke Score (PreSS) for identification and differentiation of acute stroke within 4.5 h after symptom onset.
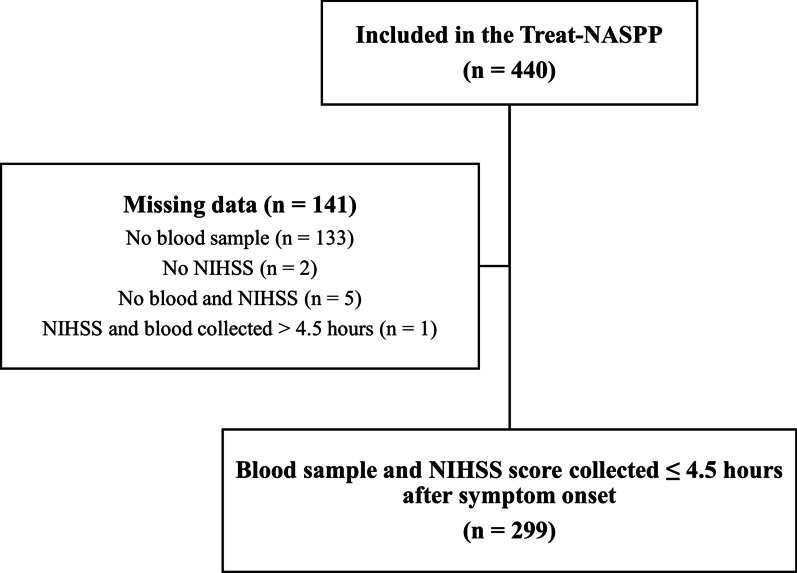
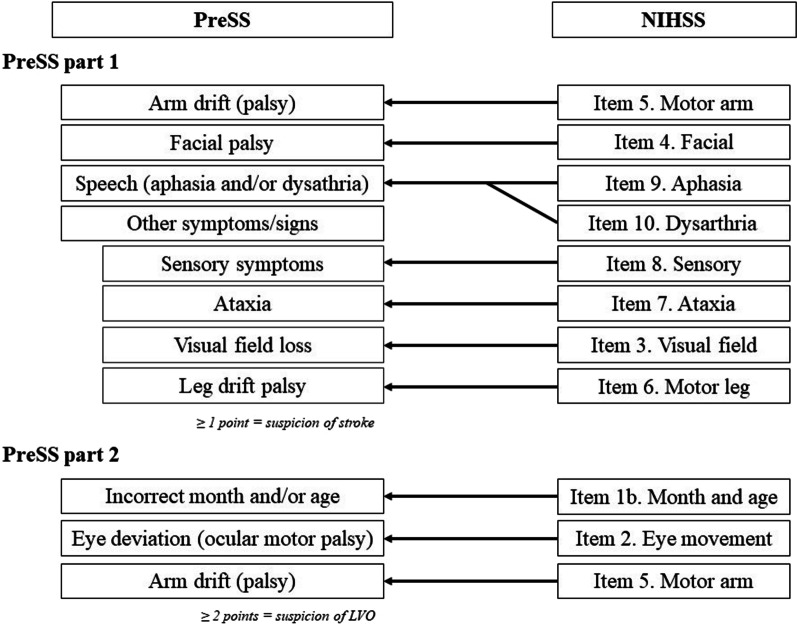
Clinical data and serum samples were collected from the Treat-Norwegian Acute Stroke Prehospital Project (Treat-NASPP). Patients with suspected stroke and symptoms lasting ≤ 4.5 h had blood samples collected and were evaluated with the National Institutes of Health Stroke Scale prospectively. In this sub study, NIHSS was retrospectively translated into PreSS and GFAP was measured using the sensitive single molecule array (SIMOA).
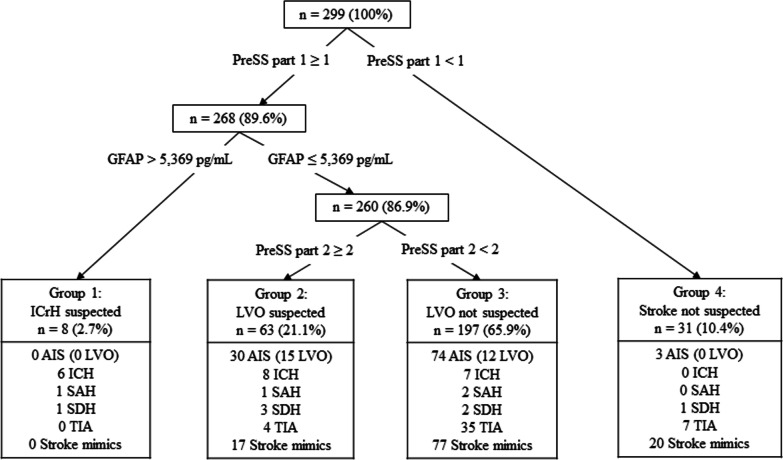
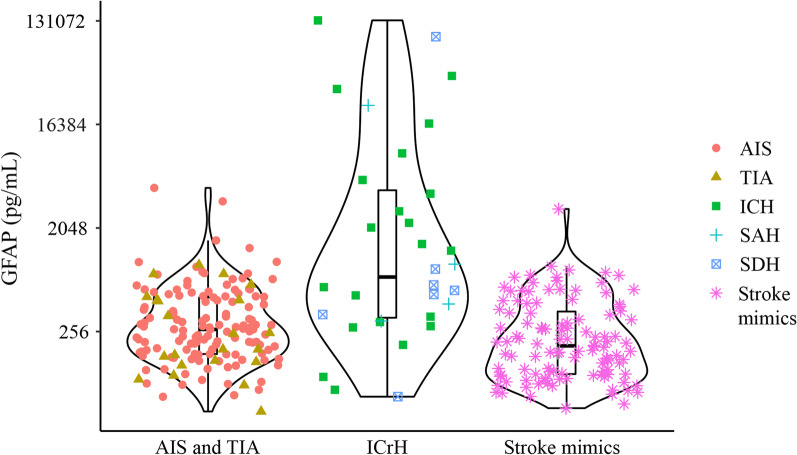
A total of 299 patients with suspected stroke were recruited from Treat-NASPP and included in this study (44% acute ischemic stroke (AIS), 10% intracranial hemorrhage (ICrH), 7% transient ischemic attack (TIA), and 38% stroke mimics). ICrH was identified with a cross-fold validated area under the receiver-operating characteristic curve (AUC) of 0.73 (95% CI 0.62-0.84). A decision tree with PreSS and GFAP combined, first identified patients with a low probability of stroke. Subsequently, GFAP detected patients with ICrH with a 25.0% sensitivity (95% CI 11.5-43.4) and 100.0% specificity (95% CI 98.6-100.0). Lastly, patients with large-vessel occlusion (LVO) were detected with a 55.6% sensitivity (95% CI 35.3-74.5) and 82.4% specificity (95% CI 77.3-86.7).
In unselected patients with suspected stroke, GFAP alone identified ICrH. Combined in a decision tree, GFAP and PreSS identified subgroups with high proportions of stroke mimics, ICrH, LVO, and AIS (non-LVO strokes).
快速识别和治疗中风对患者的预后至关重要。我们旨在确定胶质纤维酸性蛋白(GFAP)的表现,独立于并结合院前卒中评分(PreSS),以识别和区分症状发作后 4.5 小时内的急性卒中。
从治疗挪威急性卒中院前项目(Treat-NASPP)中收集临床数据和血清样本。疑似卒中且症状持续≤4.5 小时的患者采集血液样本,并前瞻性使用国立卫生研究院卒中量表(NIHSS)进行评估。在这项子研究中,NIHSS 被回顾性地转换为 PreSS,使用敏感的单分子阵列(SIMOA)测量 GFAP。
从 Treat-NASPP 招募了 299 名疑似卒中患者,纳入本研究(44%急性缺血性卒中(AIS),10%颅内出血(ICrH),7%短暂性脑缺血发作(TIA)和 38%卒中模拟)。ICrH 的交叉验证接受者操作特征曲线下面积(AUC)为 0.73(95%CI 0.62-0.84)。具有 PreSS 和 GFAP 组合的决策树首先确定卒中可能性低的患者。随后,GFAP 以 25.0%的敏感性(95%CI 11.5-43.4)和 100.0%的特异性(95%CI 98.6-100.0)检测到 ICrH。最后,使用大血管闭塞(LVO)检测到 55.6%的敏感性(95%CI 35.3-74.5)和 82.4%的特异性(95%CI 77.3-86.7)。
在未经选择的疑似卒中患者中,单独的 GFAP 可识别 ICrH。在决策树中组合使用,GFAP 和 PreSS 可识别具有较高比例卒中模拟、ICrH、LVO 和 AIS(非 LVO 卒中)的亚组。