Department of Anaesthesia and Intensive Care Medicine, School of Medicine, Clinical Sciences Institute, University of Galway, Galway University Hospital, Saolta Hospital Group, Galway, H91 YR71, Ireland.
School of Medicine, University of Galway, Galway, Ireland.
Crit Care. 2023 Jan 5;27(1):3. doi: 10.1186/s13054-022-04294-5.
Acute kidney injury (AKI) is a frequent and severe complication of both COVID-19-related acute respiratory distress syndrome (ARDS) and non-COVID-19-related ARDS. The COVID-19 Critical Care Consortium (CCCC) has generated a global data set on the demographics, management and outcomes of critically ill COVID-19 patients. The LUNG-SAFE study was an international prospective cohort study of patients with severe respiratory failure, including ARDS, which pre-dated the pandemic.
The incidence, demographic profile, management and outcomes of early AKI in patients undergoing invasive mechanical ventilation for COVID-19-related ARDS were described and compared with AKI in a non-COVID-19-related ARDS cohort.
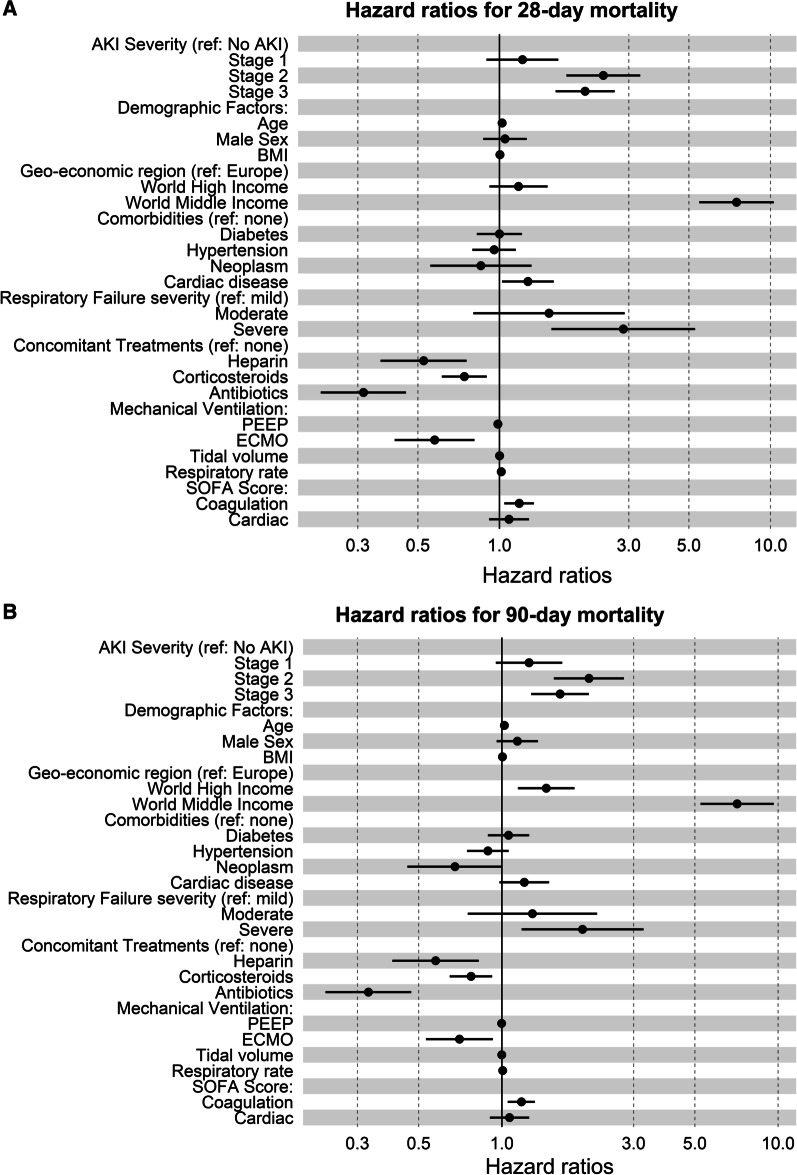
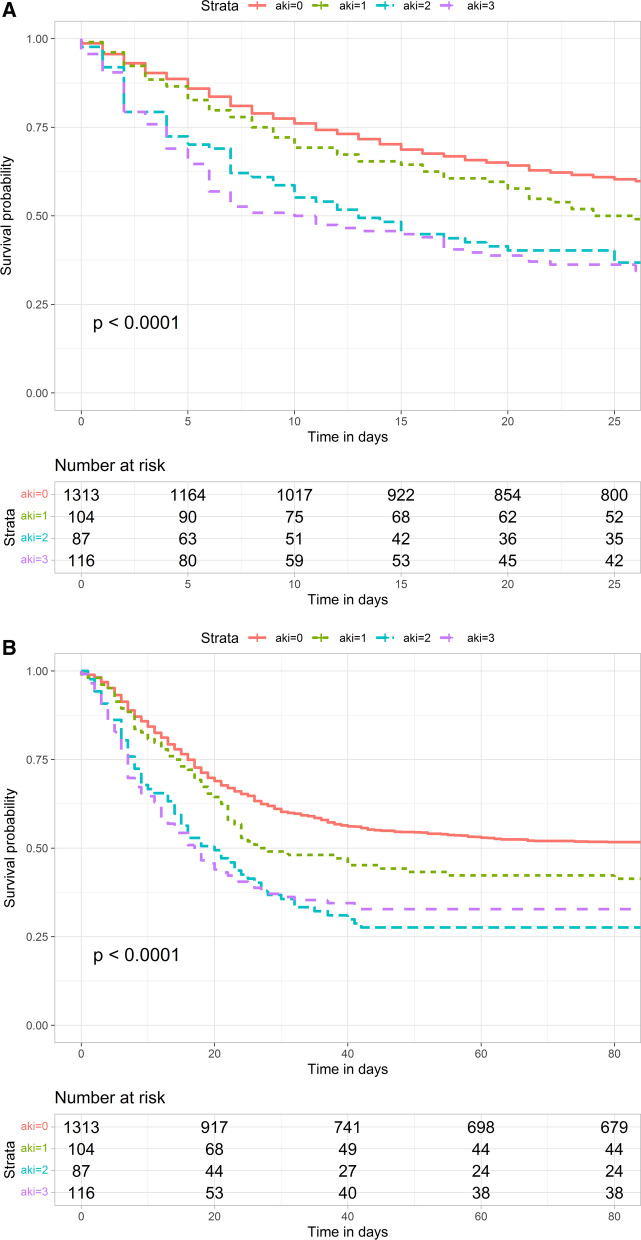
Of 18,964 patients in the CCCC data set, 1699 patients with COVID-19-related ARDS required invasive ventilation and had relevant outcome data. Of these, 110 (6.5%) had stage 1, 94 (5.5%) had stage 2, 151 (8.9%) had stage 3 AKI, while 1214 (79.1%) had no AKI within 48 h of initiating invasive mechanical ventilation. Patients developing AKI were older and more likely to have hypertension or chronic cardiac disease. There were geo-economic differences in the incidence of AKI, with lower incidence of stage 3 AKI in European high-income countries and a higher incidence in patients from middle-income countries. Both 28-day and 90-day mortality risk was increased for patients with stage 2 (HR 2.00, p < 0.001) and stage 3 AKI (HR 1.95, p < 0.001). Compared to non-COVID-19 ARDS, the incidence of shock was reduced with lower cardiovascular SOFA score across all patient groups, while hospital mortality was worse in all groups [no AKI (30 vs 50%), Stage 1 (38 vs 58%), Stage 2 (56 vs 74%), and Stage 3 (52 vs 72%), p < 0.001]. The time profile of onset of AKI also differed, with 56% of all AKI occurring in the first 48 h in patients with COVID-19 ARDS compared to 89% in the non-COVID-19 ARDS population.
AKI is a common and serious complication of COVID-19, with a high mortality rate, which differs by geo-economic location. Important differences exist in the profile of AKI in COVID-19 versus non-COVID-19 ARDS in terms of their haemodynamic profile, time of onset and clinical outcomes.
急性肾损伤(AKI)是 COVID-19 相关急性呼吸窘迫综合征(ARDS)和非 COVID-19 相关 ARDS 的常见且严重的并发症。COVID-19 重症监护联盟(CCCC)已经生成了一个关于危重症 COVID-19 患者的人口统计学、管理和结局的全球数据集。LUNG-SAFE 研究是一项针对严重呼吸衰竭患者(包括 ARDS)的国际前瞻性队列研究,该研究早于大流行之前进行。
描述了接受有创机械通气治疗 COVID-19 相关 ARDS 的患者中早期 AKI 的发生率、人口统计学特征、管理和结局,并与非 COVID-19 相关 ARDS 队列中的 AKI 进行了比较。
在 CCCC 数据集中的 18964 名患者中,有 1699 名 COVID-19 相关 ARDS 患者需要有创通气,并且有相关的结局数据。其中,110 名(6.5%)患者为 1 期 AKI,94 名(5.5%)患者为 2 期 AKI,151 名(8.9%)患者为 3 期 AKI,而 1214 名(79.1%)患者在开始有创机械通气后 48 小时内没有 AKI。发生 AKI 的患者年龄更大,更有可能患有高血压或慢性心脏疾病。AKI 的发生率存在地域经济差异,欧洲高收入国家的 3 期 AKI 发生率较低,中等收入国家的发生率较高。2 期(HR 2.00,p<0.001)和 3 期 AKI(HR 1.95,p<0.001)患者的 28 天和 90 天死亡率风险均增加。与非 COVID-19 ARDS 相比,所有患者组的心血管 SOFA 评分均较低,休克发生率降低,而所有组的住院死亡率均更差[无 AKI(30% vs 50%),1 期(38% vs 58%),2 期(56% vs 74%),3 期(52% vs 72%),p<0.001]。AKI 的发病时间也不同,COVID-19 ARDS 患者中 56%的 AKI 发生在最初 48 小时内,而非 COVID-19 ARDS 患者中 89%的 AKI 发生在最初 48 小时内。
AKI 是 COVID-19 的常见且严重的并发症,死亡率较高,且因地理位置不同而有所差异。COVID-19 与非 COVID-19 ARDS 患者的 AKI 在血流动力学特征、发病时间和临床结局方面存在重要差异。