Department of Mechanical Engineering, Michigan State University, East Lansing, MI, USA.
Department of Cardiology, University of California San Francisco, San Francisco, CA, USA.
Sci Rep. 2023 Jan 18;13(1):958. doi: 10.1038/s41598-023-28037-w.
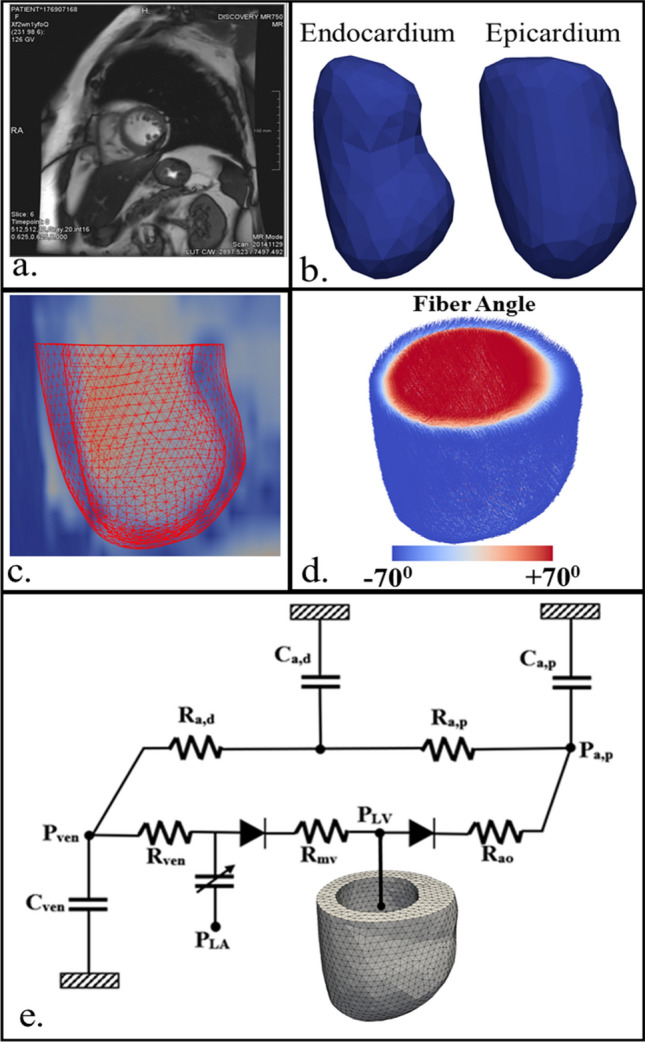
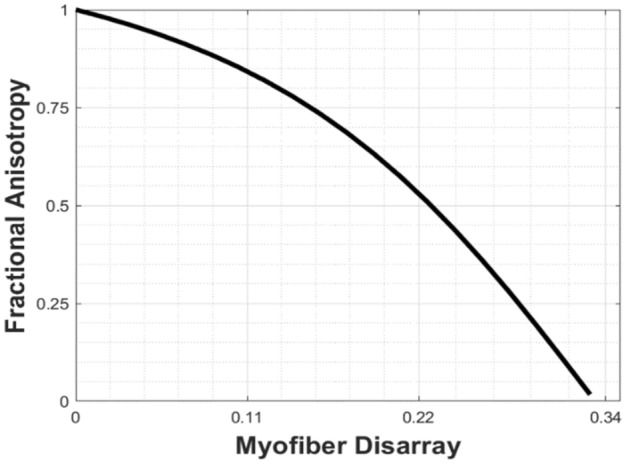
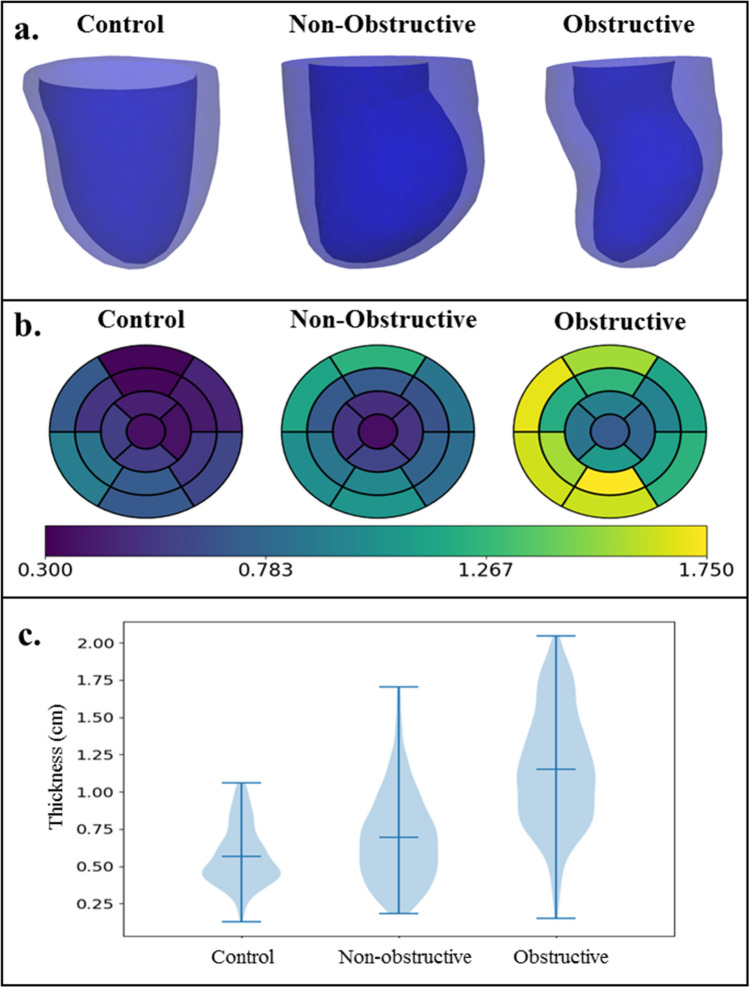
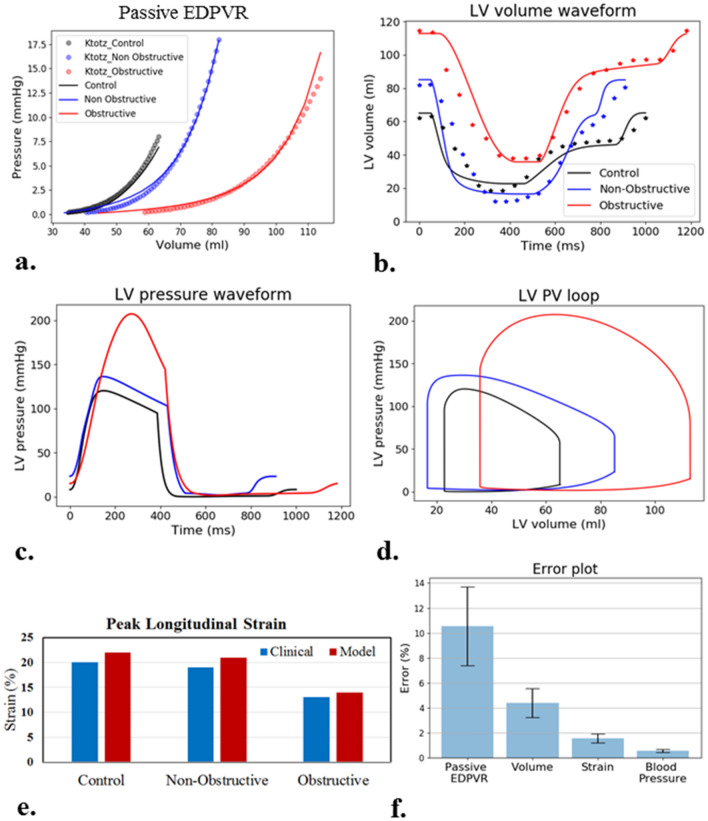
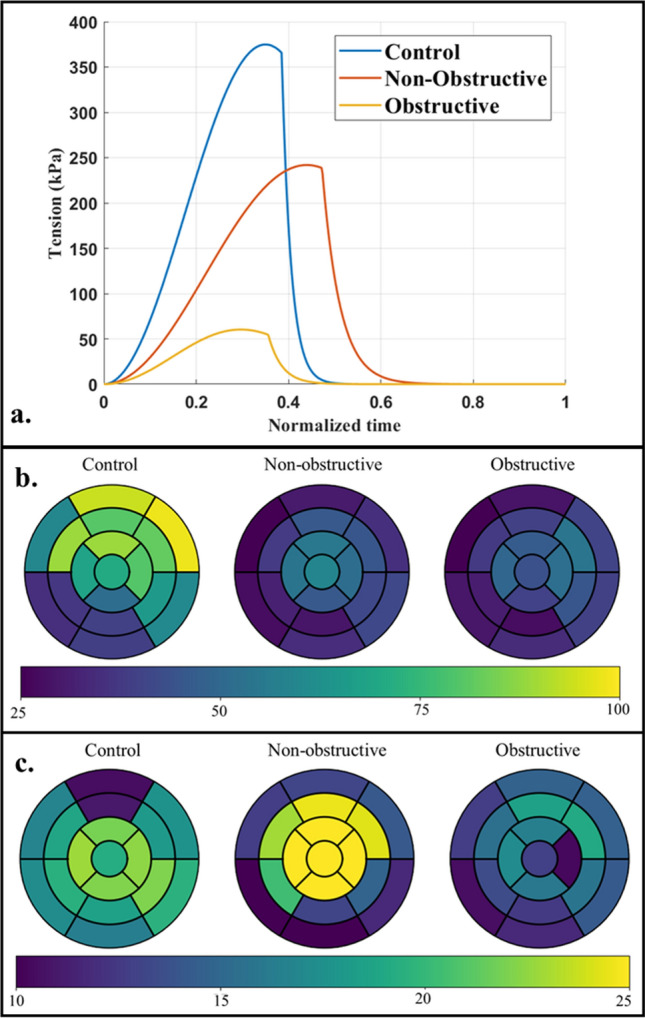
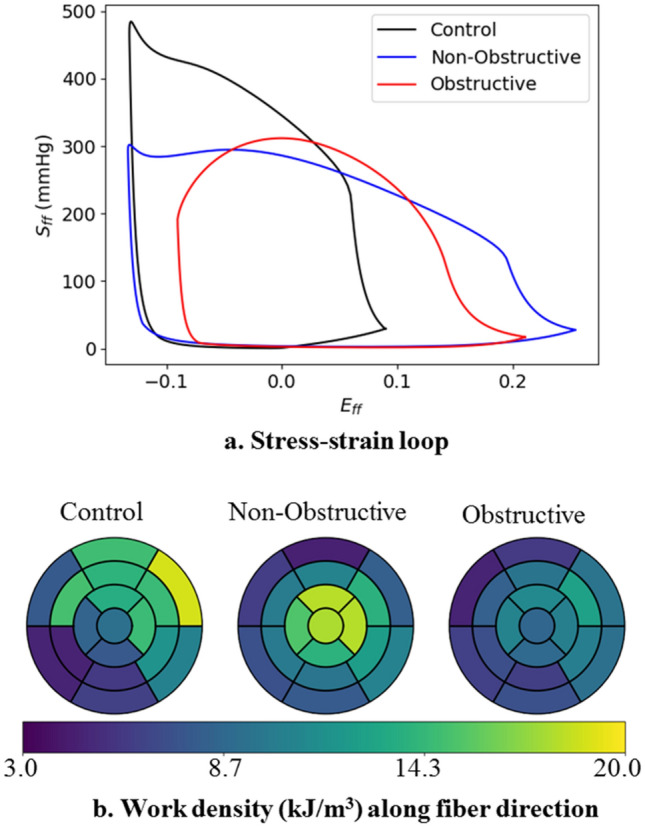
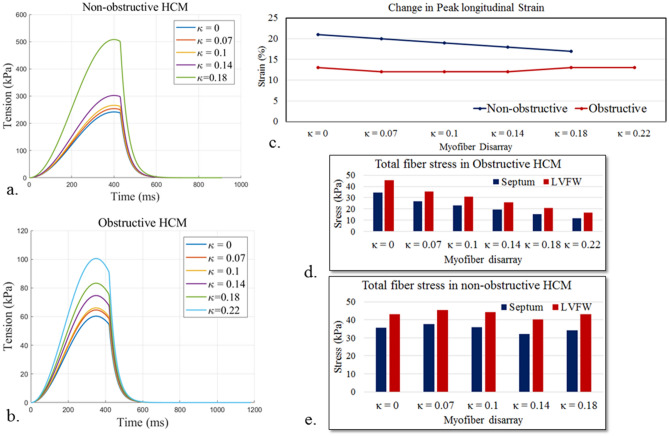
Hypertrophic cardiomyopathy (HCM) is a genetic heart disease that is associated with many pathological features, such as a reduction in global longitudinal strain (GLS), myofiber disarray and hypertrophy. The effects of these features on left ventricle (LV) function are, however, not clear in two phenotypes of HCM, namely, obstructive and non-obstructive. To address this issue, we developed patient-specific computational models of the LV using clinical measurements from 2 female HCM patients and a control subject. Left ventricular mechanics was described using an active stress formulation and myofiber disarray was described using a structural tensor in the constitutive models. Unloaded LV configuration for each subject was first determined from their respective end-diastole LV geometries segmented from the cardiac magnetic resonance images, and an empirical single-beat estimation of the end-diastolic pressure volume relationship. The LV was then connected to a closed-loop circulatory model and calibrated using the clinically measured LV pressure and volume waveforms, peak GLS and blood pressure. Without consideration of myofiber disarray, peak myofiber tension was found to be lowest in the obstructive HCM subject (60 kPa), followed by the non-obstructive subject (242 kPa) and the control subject (375 kPa). With increasing myofiber disarray, we found that peak tension has to increase in the HCM models to match the clinical measurements. In the obstructive HCM patient, however, peak tension was still depressed (cf. normal subject) at the largest degree of myofiber disarray found in the clinic. The computational modeling workflow proposed here can be used in future studies with more HCM patient data.
肥厚型心肌病(HCM)是一种遗传性心脏病,与许多病理特征相关,如整体纵向应变(GLS)降低、肌纤维排列紊乱和肥大。然而,在 HCM 的两种表型,即梗阻性和非梗阻性中,这些特征对左心室(LV)功能的影响尚不清楚。为了解决这个问题,我们使用来自 2 名女性 HCM 患者和 1 名对照患者的临床测量值,为 LV 开发了特定于患者的计算模型。使用主动应力公式描述 LV 力学,在本构模型中使用结构张量描述肌纤维排列紊乱。首先从心脏磁共振图像分割的各自的 LV 舒张末期几何形状确定每个受试者的 LV 无载配置,然后对舒张末期压力-容积关系进行经验单拍估计。然后将 LV 与闭环循环模型连接,并使用临床测量的 LV 压力和容积波形、GLS 峰值和血压进行校准。不考虑肌纤维排列紊乱时,发现梗阻性 HCM 患者的峰值肌纤维张力最低(60kPa),其次是非梗阻性患者(242kPa)和对照组(375kPa)。随着肌纤维排列紊乱的增加,我们发现 HCM 模型中的峰值张力必须增加才能与临床测量值匹配。然而,在梗阻性 HCM 患者中,在临床中发现的最大程度的肌纤维排列紊乱下,峰值张力仍然降低(与正常受试者相比)。这里提出的计算建模工作流程可用于未来有更多 HCM 患者数据的研究。