Mackinnon Erin S, Har Bryan, Champsi Salimah, Wani Rajvi J, Geyer Lee, Shaw Eileen, Farris Megan S, Anderson Todd J
Amgen Canada Inc., 6775 Financial Dr #100, Mississauga, ON, L5N 0A4, Canada.
Libin Cardiovascular Institute, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada.
Cardiol Ther. 2023 Jun;12(2):327-338. doi: 10.1007/s40119-022-00300-7. Epub 2023 Jan 19.
A high proportion of Canadian patients with acute myocardial infarction (AMI) do not achieve the threshold low-density lipoprotein cholesterol (LDL-C) levels recommended by the Canadian Cardiovascular Society in 2021. This increases the risk of subsequent atherosclerotic cardiovascular disease (ASCVD) events. Here, we assess LDL-C levels and threshold achievement among patients by lipid-lowering therapies (LLT) received post-AMI.
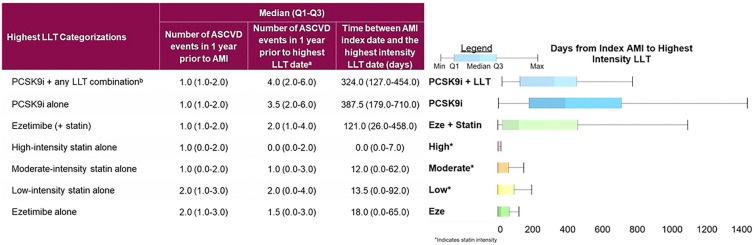
A retrospective cohort study of patients identified with AMI between 2015 and 2019 was conducted using administrative health databases in Alberta, Canada. Patients were grouped by their highest-intensity LLT post-AMI (proprotein convertase subtilisin/kexin type 9 inhibitors (PCSK9i) + another LLT; PCSK9i alone; ezetimibe + statin; statins (high, moderate, low intensity); or ezetimibe alone), and available LDL-C levels were examined in the year before and after LLT dispense date.
The cohort included 15,283 patients. In patients on PCSK9i + LLT, the median [95% confidence interval (CI)] LDL-C levels decreased from 2.7 (2.3-3.4) before to 0.9 (0.5-1.2) mmol/l after treatment, the largest decrease among treatment groups. In the ezetimibe + statin and high-intensity statin groups, median (95% CI) values after treatment were 1.5 (1.5-1.6) and 1.4 (1.4-1.4) mmol/l, respectively. The proportion of patients below the 1.8 mmol/l threshold increased by 77.7% in the PSCK9i + LLT group after treatment, compared to 45.4 and 32.4% in the ezetimibe + statin and high-intensity statin groups, respectively.
Intensification with PCSK9i in AMI patients results in a greater proportion of patients achieving below the recommended LDL-C threshold versus statins and or ezetimibe alone. Increased focus on achieving below the LDL-C thresholds with additional LLT as required may benefit patient cardiovascular outcomes.
很大一部分加拿大急性心肌梗死(AMI)患者未达到加拿大心血管学会2021年推荐的低密度脂蛋白胆固醇(LDL-C)阈值水平。这增加了后续动脉粥样硬化性心血管疾病(ASCVD)事件的风险。在此,我们评估AMI后接受降脂治疗(LLT)的患者的LDL-C水平及阈值达标情况。
利用加拿大艾伯塔省的行政卫生数据库,对2015年至2019年间确诊为AMI的患者进行了一项回顾性队列研究。患者按AMI后接受的最高强度LLT分组(前蛋白转化酶枯草溶菌素/kexin 9型抑制剂(PCSK9i)+另一种LLT;单独使用PCSK9i;依折麦布+他汀类药物;他汀类药物(高强度、中等强度、低强度);或单独使用依折麦布),并在LLT配药日期前后一年检查可用的LDL-C水平。
该队列包括15283名患者。接受PCSK9i+LLT治疗的患者中,LDL-C水平中位数[95%置信区间(CI)]从治疗前的2.7(2.3 - 3.4)mmol/L降至治疗后的0.9(0.5 - 1.2)mmol/L,是各治疗组中下降幅度最大的。在依折麦布+他汀类药物组和高强度他汀类药物组中,治疗后的中位数(95%CI)值分别为1.5(1.5 - 1.6)mmol/L和1.4(1.4 - 1.4)mmol/L。治疗后,PCSK9i+LLT组中LDL-C水平低于1.8 mmol/L阈值的患者比例增加了77.7%,相比之下,依折麦布+他汀类药物组和高强度他汀类药物组分别为45.4%和32.4%。
与单独使用他汀类药物和/或依折麦布相比,AMI患者强化使用PCSK9i可使更多患者达到推荐的LDL-C阈值以下。根据需要增加使用其他LLT以达到LDL-C阈值以下,可能会改善患者的心血管结局。