1Steno Diabetes Center Copenhagen, Herlev, Denmark.
2Department of Clinical Pharmacy and Pharmacology, University of Groningen, Groningen, the Netherlands.
Diabetes Care. 2023 Mar 1;46(3):593-601. doi: 10.2337/dc22-1699.
Renin-angiotensin system (RAS) inhibitors decrease the urinary albumin to creatinine ratio (UACR) but are ineffective in up to 40% of patients. We hypothesized that rotation through different drug classes overcomes RAS inhibitor resistance and tested this in a randomized crossover trial.
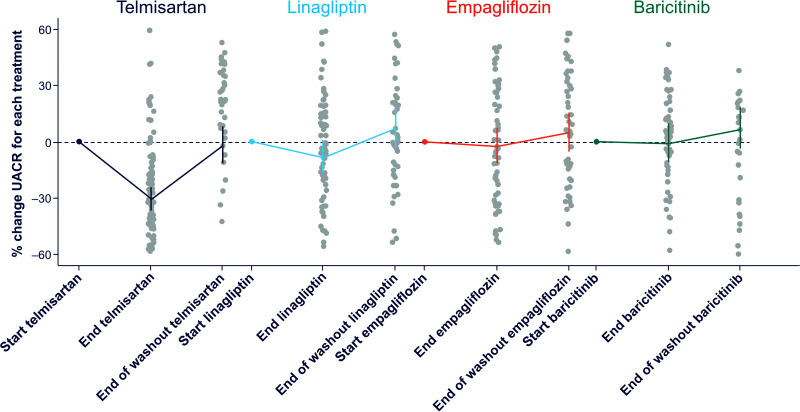
We assigned 26 adults with type 1 diabetes and 37 with type 2 diabetes and UACR between 30 and 500 mg/g and estimated glomerular filtration rate >45 mL/min/1.73 m2 to 4-week treatment periods with telmisartan 80 mg, empagliflozin 10 mg, linagliptin 5 mg, and baricitinib 2 mg in random order, separated by 4-week washout periods. Each participant was then re-exposed for 4 weeks to the drug that induced that individual's largest UACR reduction. Primary outcome was the difference in UACR response to the best-performing drug during the confirmation period versus UACR response to the other three drugs.
There was substantial variation in the best-performing drug. Telmisartan was best performing for 33 participants (52%), empagliflozin and linagliptin in 11 (17%), and baricitinib in 8 participants (13%). The individuals' best-performing drug changed UACR from baseline during the first and confirmatory exposures by a mean of -39.6% (95% CI -44.8, -33.8; P < 0.001) and -22.4% (95% CI -29.7, -12.5; P < 0.001), respectively. The Pearson correlation for first versus confirmatory exposure was 0.39 (P = 0.017). The mean change in UACR with the other three drugs was +1.6% (95% CI -4.3%, 8.0%; P = 0.593 versus baseline; difference versus individuals' best-performing drug at confirmation, 30.9% [95% CI 18.0, 45.3]; P < 0.001).
We demonstrated a large and reproducible variation in participants' responses to different UACR-lowering drug classes. These data support systematic rotation through different drug classes to overcome therapy resistance to RAS inhibition.
肾素-血管紧张素系统(RAS)抑制剂可降低尿白蛋白与肌酐比值(UACR),但在多达 40%的患者中无效。我们假设通过不同药物类别轮换可以克服 RAS 抑制剂的耐药性,并在一项随机交叉试验中对此进行了测试。
我们将 26 名 1 型糖尿病患者和 37 名 2 型糖尿病患者以及 UACR 在 30 至 500 mg/g 之间且估计肾小球滤过率 >45 mL/min/1.73 m2 的患者分配至为期 4 周的治疗期,分别接受替米沙坦 80 mg、恩格列净 10 mg、利格列汀 5 mg 和巴利替尼 2 mg 治疗,随机顺序排列,并用 4 周洗脱期隔开。然后,每位参与者再接受为期 4 周的治疗,药物为在确认期内诱导 UACR 降低最多的药物。主要结局是在确认期内最佳表现药物的 UACR 反应与其他三种药物的 UACR 反应之间的差异。
最佳表现药物的变化幅度很大。替米沙坦对 33 名参与者(52%)、恩格列净和利格列汀对 11 名参与者(17%)、巴利替尼对 8 名参与者(13%)的表现最佳。个体的最佳表现药物在第一次和确认暴露期间使 UACR 从基线降低了 -39.6%(95%CI -44.8,-33.8;P < 0.001)和 -22.4%(95%CI -29.7,-12.5;P < 0.001),分别。第一次与确认暴露的 Pearson 相关性为 0.39(P = 0.017)。其他三种药物的 UACR 平均变化为 +1.6%(95%CI -4.3%,8.0%;P = 0.593 与基线相比;与个体最佳表现药物在确认时的差异为 30.9%[95%CI 18.0,45.3];P < 0.001)。
我们证明了参与者对不同 UACR 降低药物类别的反应存在很大且可重复的差异。这些数据支持系统地轮换使用不同的药物类别以克服对 RAS 抑制的治疗耐药性。