Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA.
Department of Clinical Pharmacy and Pharmacology, University of Groningen, University Medical Center Groningen, Groningen, Netherlands.
Lancet Diabetes Endocrinol. 2019 Feb;7(2):115-127. doi: 10.1016/S2213-8587(18)30313-9. Epub 2019 Jan 8.
Change in albuminuria as a surrogate endpoint for progression of chronic kidney disease is strongly supported by biological plausibility, but empirical evidence to support its validity in epidemiological studies is lacking. We aimed to assess the consistency of the association between change in albuminuria and risk of end-stage kidney disease in a large individual participant-level meta-analysis of observational studies.
In this meta-analysis, we collected individual-level data from eligible cohorts in the Chronic Kidney Disease Prognosis Consortium (CKD-PC) with data on serum creatinine and change in albuminuria and more than 50 events on outcomes of interest. Cohort data were eligible if participants were aged 18 years or older, they had a repeated measure of albuminuria during an elapsed period of 8 months to 4 years, subsequent end-stage kidney disease or mortality follow-up data, and the cohort was active during this consortium phase. We extracted participant-level data and quantified percentage change in albuminuria, measured as change in urine albumin-to-creatinine ratio (ACR) or urine protein-to-creatinine ratio (PCR), during baseline periods of 1, 2, and 3 years. Our primary outcome of interest was development of end-stage kidney disease after a baseline period of 2 years. We defined an end-stage kidney disease event as initiation of kidney replacement therapy. We quantified associations of percentage change in albuminuria with subsequent end-stage kidney disease using Cox regression in each cohort, followed by random-effects meta-analysis. We further adjusted for regression dilution to account for imprecision in the estimation of albuminuria at the participant level. We did multiple subgroup analyses, and also repeated our analyses using participant-level data from 14 clinical trials, including nine clinical trials not in CKD-PC.
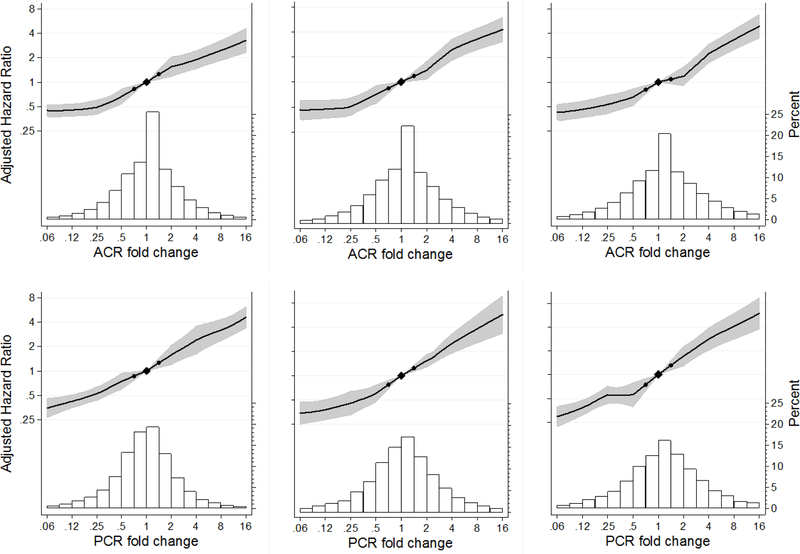
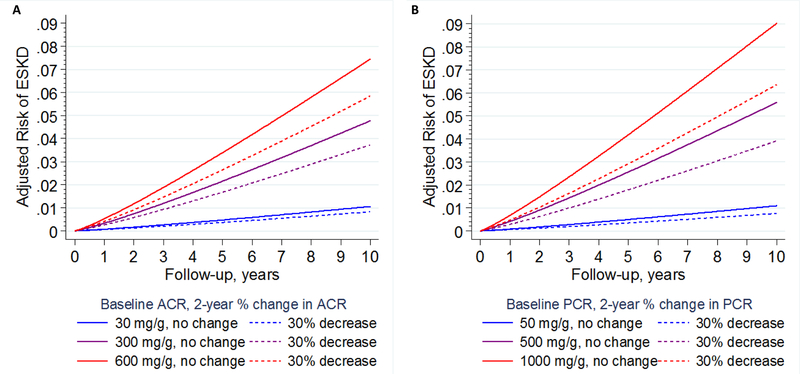
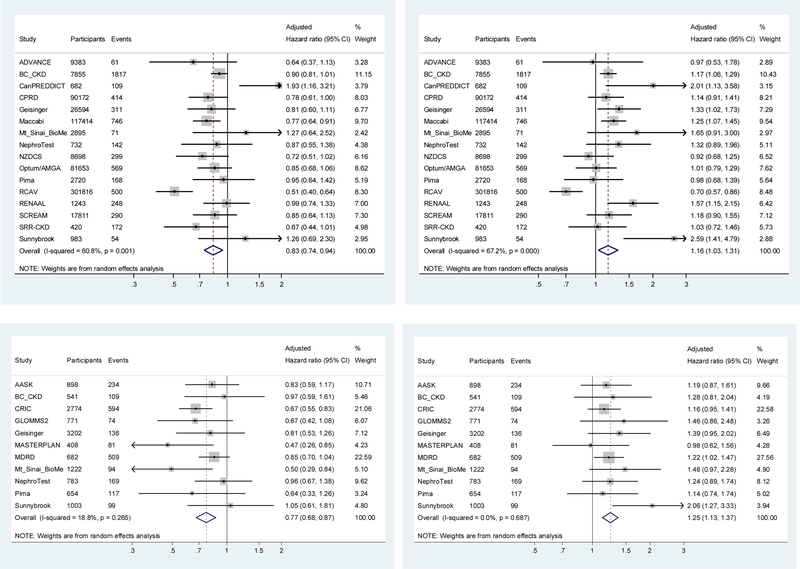
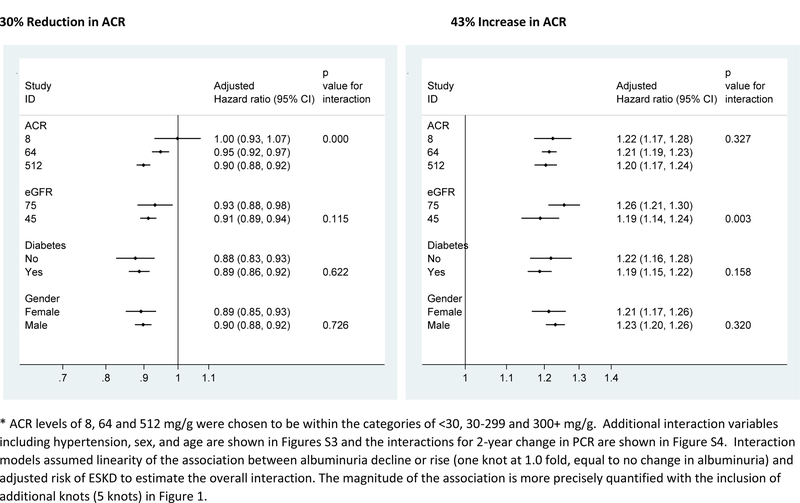
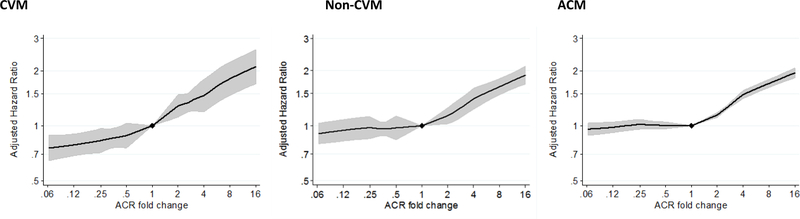
Between July, 2015, and June, 2018, we transferred and analysed data from 28 cohorts in the CKD-PC, which included 693 816 individuals (557 583 [80%] with diabetes). Data for 675 904 individuals and 7461 end-stage kidney disease events were available for our primary outcome analysis. Change in ACR was consistently associated with subsequent risk of end-stage kidney disease. The adjusted hazard ratio (HR) for end-stage kidney disease after a 30% decrease in ACR during a baseline period of 2 years was 0·83 (95% CI 0·74-0·94), decreasing to 0·78 (0·66-0·92) after further adjustment for regression dilution. Adjusted HRs were fairly consistent across cohorts and subgroups (ie, estimated glomerular filtration rate, diabetes, and sex), but the association was somewhat stronger among participants with higher baseline ACR than among those with lower baseline ACR (p<0·0001). In individuals with baseline ACR of 300 mg/g or higher, a 30% decrease in ACR over 2 years was estimated to confer a more than 1% absolute reduction in 10-year risk of end-stage kidney disease, even at early stages of chronic kidney disease. Results were generally similar when we used change in PCR and when study populations from clinical trials were assessed.
Change in albuminuria was consistently associated with subsequent risk of end-stage kidney disease across a range of cohorts, lending support to the use of change in albuminuria as a surrogate endpoint for end-stage kidney disease in clinical trials of progression of chronic kidney disease in the setting of increased albuminuria.
US National Kidney Foundation and US National Institute of Diabetes and Digestive and Kidney Diseases.
白蛋白尿的变化作为慢性肾脏病进展的替代终点,具有很强的生物学合理性,但缺乏在流行病学研究中支持其有效性的经验证据。我们旨在通过慢性肾脏病预后联盟(CKD-PC)中大型个体参与者水平荟萃分析评估白蛋白尿变化与终末期肾病风险之间的一致性关联,该分析纳入了观察性研究中的个体数据。
在这项荟萃分析中,我们从 CKD-PC 中符合条件的队列中收集个体数据,这些队列的数据包括血清肌酐和白蛋白尿变化以及超过 50 个感兴趣结局的事件。如果参与者年龄在 18 岁或以上,在 8 个月至 4 年的时间内重复测量白蛋白尿,随后有终末期肾病或死亡率随访数据,并且在本联盟阶段期间队列活跃,那么队列数据是合格的。我们提取了参与者水平的数据,并量化了白蛋白尿的百分比变化,通过尿液白蛋白/肌酐比(ACR)或尿液蛋白/肌酐比(PCR)的变化来衡量,基线期为 1、2 和 3 年。我们的主要结局是在基线期 2 年后发生终末期肾病。我们将终末期肾病事件定义为开始进行肾脏替代治疗。我们使用每个队列中的 Cox 回归来量化白蛋白尿变化与随后的终末期肾病之间的关联,然后进行随机效应荟萃分析。我们进一步调整了回归稀释,以考虑到参与者水平白蛋白尿估计的不准确性。我们进行了多项亚组分析,还使用包括 14 项临床试验在内的 14 项临床试验的参与者水平数据重复了我们的分析,其中包括 9 项不在 CKD-PC 中的临床试验。
在 2015 年 7 月至 2018 年 6 月期间,我们转移并分析了 CKD-PC 中 28 个队列的数据,这些队列包括 693816 个人(557583[80%]患有糖尿病)。我们的主要结局分析可获得 675904 名个人和 7461 例终末期肾病事件的数据。在基线期 2 年内 ACR 下降 30%后,发生终末期肾病的调整后的危险比(HR)为 0.83(95%CI 0.74-0.94),进一步调整回归稀释后下降至 0.78(0.66-0.92)。调整后的 HR 在队列和亚组之间相当一致(即估计肾小球滤过率、糖尿病和性别),但在基线 ACR 较高的参与者中,该关联强于基线 ACR 较低的参与者(p<0.0001)。在基线 ACR 为 300mg/g 或更高的个体中,估计在 2 年内 ACR 下降 30%可使终末期肾病 10 年风险降低超过 1%,即使在慢性肾脏病的早期阶段也是如此。当我们使用 PCR 变化和评估临床试验人群时,结果基本相似。
白蛋白尿的变化与一系列队列中随后的终末期肾病风险之间存在一致关联,这支持在白蛋白尿升高的情况下,将白蛋白尿变化作为终末期肾病进展的临床试验中的替代终点。
美国国家肾脏基金会和美国国家糖尿病、消化和肾脏疾病研究所。