Children's Hospital of Philadelphia, Philadelphia, PA 19104, USA.
Department of Pediatrics, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA 19104, USA.
Genes (Basel). 2022 Dec 24;14(1):62. doi: 10.3390/genes14010062.
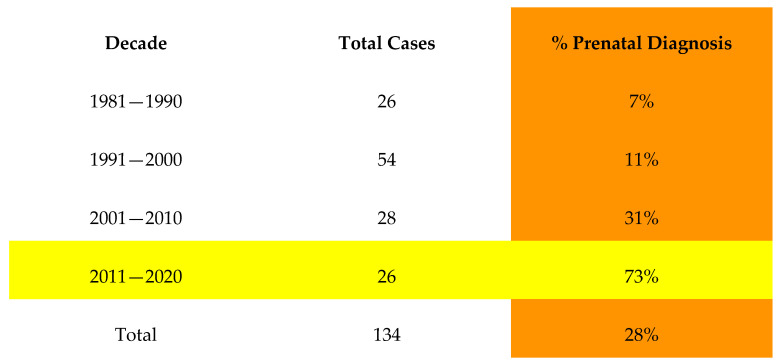
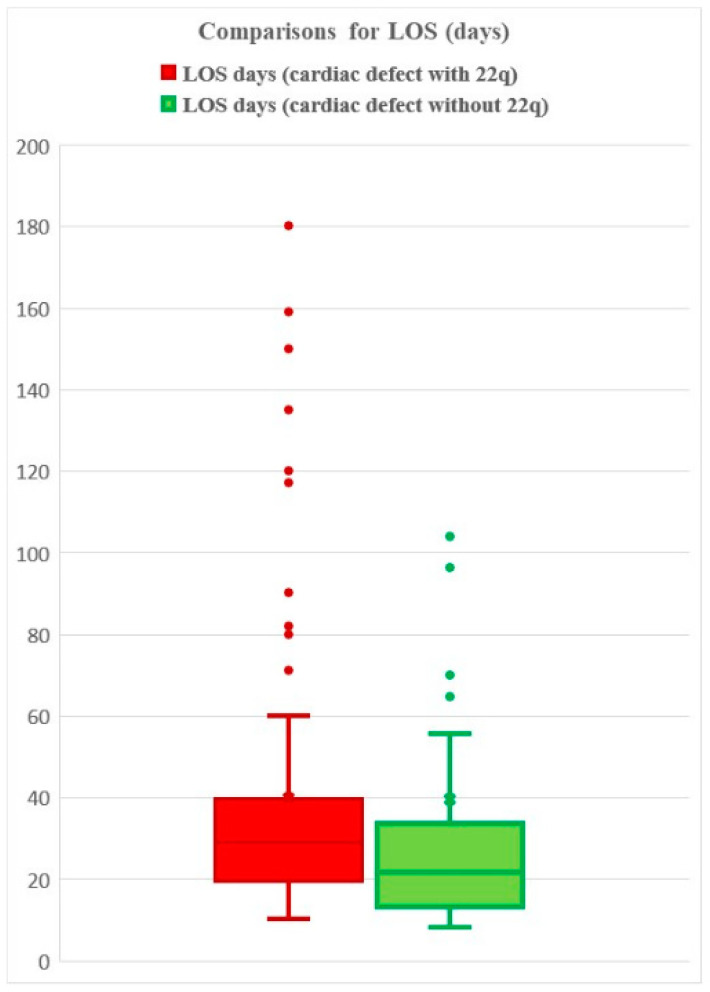
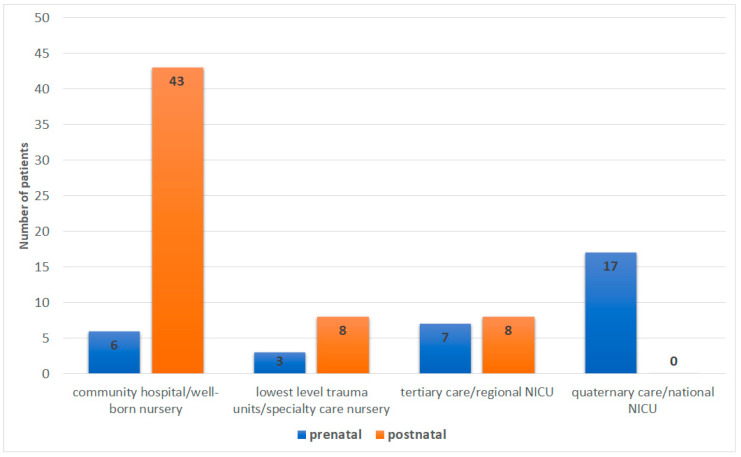
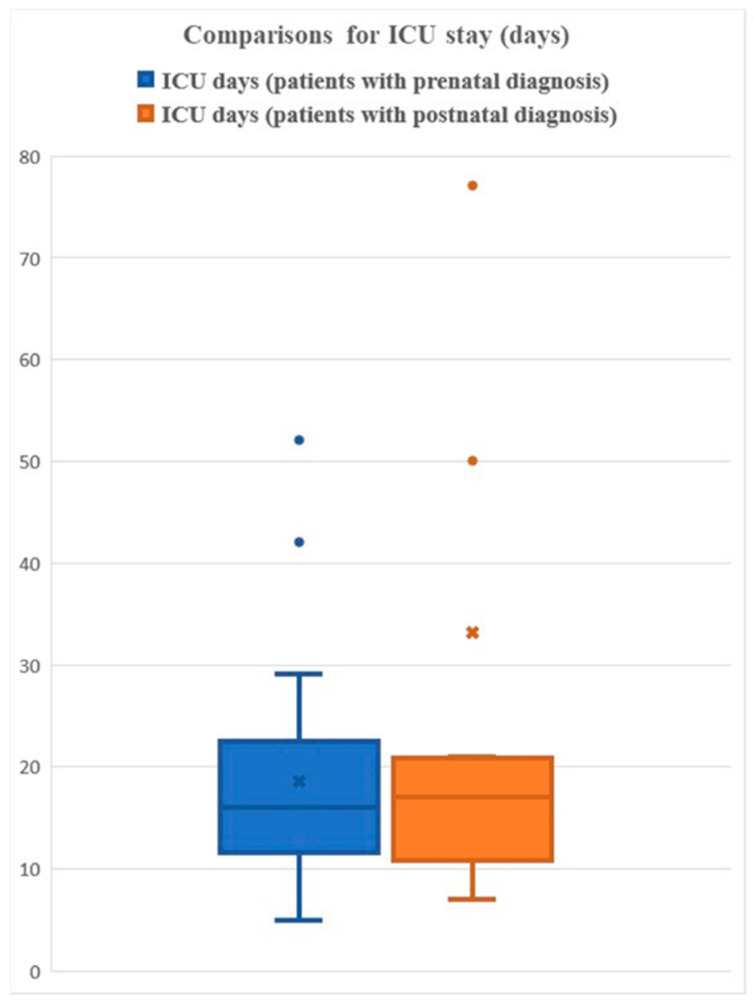
Interruption of the aortic arch (IAA) is a rare but life-threatening congenital heart defect if not corrected in the neonatal period. IAA type B is highly correlated with 22q11.2 deletion syndrome (22q11.2DS); approximately 50% of patients with IAA type B also have 22q11.2DS (Peyvandi et al.; Goldmuntz et al.). Early identification and repair of IAA can prevent severe morbidity and death. However, IAA is challenging to identify prenatally, or even in the neonatal period. In this study, we examined infants with IAA, diagnosed during pregnancy and prior to discharge (PPTD) from the birth hospital vs. those diagnosed following discharge (FD) from the newborn nursery. Our goals were to determine: (1) if early diagnosis improved outcomes; and (2) if patients with IAA and without 22q11.2DS had similar outcomes. In total, 135 patients with a diagnosis of 22q11.2DS and IAA were ascertained through the 22q and You Center at the Children's Hospital of Philadelphia (CHOP). The examined outcomes included: timing of diagnosis; age at diagnosis (days); hospital length of stay (LOS); duration of intensive care unit (ICU) stay; mechanical ventilation (days); duration of inotrope administration (days); year of surgical intervention; birth hospital trauma level; and overall morbidity. These outcomes were then compared with 40 CHOP patients with IAA but without 22q11.2DS. The results revealed that the PPTD neonates had fewer days of intubation, inotrope administration, and hospital LOS when compared to the FD group. The outcomes between deleted and non-deleted individuals with IAA differed significantly, in terms of the LOS (40 vs. 39 days) and time in ICU (28 vs. 24 days), respectively. These results support the early detection of 22q11.2DS via prenatal screening/diagnostics/newborn screening, as IAA can evade routine prenatal ultrasound and postnatal pulse oximetry. However, as previously reported in patients with 22q11.2DS and congenital heart disease (CHD), patients with 22q11.2DS tend to fare poorer compared to non-deleted neonates with IAA.
主动脉弓中断(IAA)是一种罕见但危及生命的先天性心脏病,如果不在新生儿期得到纠正,后果将十分严重。IAA 型 B 与 22q11.2 缺失综合征(22q11.2DS)高度相关;大约 50%的 IAA 型 B 患者也有 22q11.2DS(Peyvandi 等人;Goldmuntz 等人)。早期识别和修复 IAA 可以预防严重的发病率和死亡率。然而,IAA 在产前甚至新生儿期都很难识别。在这项研究中,我们研究了在出生医院(PPTD)诊断出患有 IAA 的婴儿,与在新生儿重症监护室(FD)诊断出患有 IAA 的婴儿进行比较。我们的目标是确定:(1)早期诊断是否改善了结局;(2)是否患有 IAA 但无 22q11.2DS 的患者的结局相似。总共有 135 名被诊断为 22q11.2DS 和 IAA 的患者通过费城儿童医院的 22q 和 You 中心确定(CHOP)。检查的结果包括:诊断时间;诊断时的年龄(天);住院时间(LOS);重症监护病房(ICU)停留时间;机械通气(天);去甲肾上腺素给药时间(天);手术干预的年份;出生医院创伤等级;以及整体发病率。然后将这些结果与 40 名在 CHOP 医院被诊断为 IAA 但无 22q11.2DS 的患者进行比较。结果表明,与 FD 组相比,PPTD 新生儿的插管天数、去甲肾上腺素给药天数和住院 LOS 天数更少。患有 IAA 的删除和未删除个体之间的结果存在显著差异,在 LOS(40 天与 39 天)和 ICU 时间(28 天与 24 天)方面。这些结果支持通过产前筛查/诊断/新生儿筛查早期发现 22q11.2DS,因为 IAA 可以逃避常规产前超声和产后脉搏血氧饱和度检查。然而,正如先前报道的患有 22q11.2DS 和先天性心脏病(CHD)的患者一样,患有 22q11.2DS 的患者的预后比非删除的 IAA 新生儿差。