Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, New York.
Department of Radiation Oncology, University of Texas MD Anderson Cancer Center, Houston, Texas.
JAMA Netw Open. 2023 Jan 3;6(1):e2250607. doi: 10.1001/jamanetworkopen.2022.50607.
Use of proton therapy reirradiation (PT-ReRT) for head and neck cancer is increasing; however, reports are heterogenous and outcomes can be difficult to interpret.
To evaluate outcomes and toxic effects following PT-ReRT in a uniform and consecutive cohort of patients with head and neck squamous cell carcinoma.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study included patients with recurrent primary head and neck squamous cell carcinoma who were treated with PT-ReRT from January 1, 2013, to December 31, 2020, at a single institution. Patient, clinical, and treatment characteristics were obtained, and multidisciplinary review was performed to record and grade early and late toxic effects.
Proton therapy reirradiation.
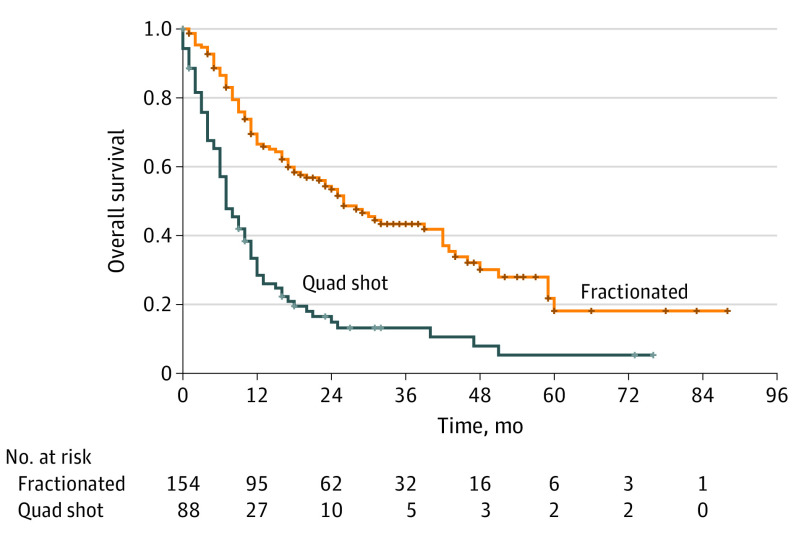
Follow-up was defined from the start of PT-ReRT. The Kaplan-Meier method was used for outcomes of interest, including local control (LC), locoregional control, distant metastatic control, progression-free survival, and overall survival (OS). Cox proportional hazards regression modeling was used to assess associations of covariates with OS.
A total of 242 patients (median [range] age, 63 [21-96] years; 183 [75.6%] male) were included. Of these patients, 231 (95.9%) had a Karnofsky performance status score of 70 or higher, and 145 (59.9%) had at least a 10-pack-year smoking history. Median (range) follow-up was 12.0 (5.8-26.0) months for all patients and 24.5 (13.8-37.8) months for living patients. A total of 206 patients (85.1%) had recurrent disease vs second primary or residual disease. The median (range) interval between radiation courses was 22 (1-669) months. Median PT-ReRT dose was 70 cobalt gray equivalents (CGE) for the fractionated cohort and 44.4 CGE for the quad shot cohort. For the fractionated cohort, the 1-year LC was 71.8% (95% CI, 62.8%-79.0%) and the 1-year OS was 66.6% (95% CI, 58.1%-73.8%). For the quad shot cohort, the 1-year LC was 61.6% (95% CI, 46.4%-73.6%) and the 1-year OS was 28.5% (95% CI, 19.4%-38.3%). Higher Karnofsky performance status scores (hazard ratio [HR], 0.50; 95% CI, 0.25-0.99; P = .046) and receipt of salvage surgery prior to PT-ReRT (HR, 0.57; 95% CI, 0.39-0.84; P = .005) were associated with improved OS, whereas receipt of quad shot (HR, 1.97; 95% CI, 1.36-2.86; P < .001) was associated with worse OS. There were a total of 73 grade 3 and 6 grade 4 early toxic effects. There were 79 potential grade 3, 4 grade 4, and 5 grade 5 late toxic effects.
The findings of this cohort study suggest that, compared with previous reports with photon-based reirradiation, patients are living longer with aggressive PT-ReRT; however, surviving patients remain at risk of early and late complications.
质子治疗再放疗(PT-ReRT)在头颈部癌症中的应用正在增加;然而,报告结果存在异质性,且结果难以解释。
评估在头颈部鳞状细胞癌的统一和连续队列中,使用质子治疗再放疗的结果和毒副作用。
设计、地点和参与者:本回顾性队列研究纳入了 2013 年 1 月 1 日至 2020 年 12 月 31 日在一家机构接受复发性头颈部原发性鳞状细胞癌 PT-ReRT 的患者。获取患者、临床和治疗特征,并进行多学科审查以记录和分级早期和晚期毒性作用。
质子治疗再放疗。
随访从 PT-ReRT 开始计算。使用 Kaplan-Meier 方法评估感兴趣的结局,包括局部控制(LC)、局部区域控制、远处转移控制、无进展生存和总生存(OS)。使用 Cox 比例风险回归模型评估协变量与 OS 的相关性。
共纳入 242 例患者(中位[范围]年龄,63[21-96]岁;183[75.6%]为男性)。其中,231 例(95.9%)的 Karnofsky 表现状态评分为 70 或更高,145 例(59.9%)有至少 10 包年的吸烟史。所有患者的中位(范围)随访时间为 12.0(5.8-26.0)个月,生存患者的中位随访时间为 24.5(13.8-37.8)个月。206 例(85.1%)患者为复发性疾病,20 例(8.3%)为第二原发或残留疾病。放疗之间的中位(范围)间隔为 22(1-669)个月。中位 PT-ReRT 剂量为分次照射队列的 70 钴格雷等效物(CGE)和四分体照射队列的 44.4 CGE。在分次照射队列中,1 年 LC 为 71.8%(95%CI,62.8%-79.0%),1 年 OS 为 66.6%(95%CI,58.1%-73.8%)。在四分体照射队列中,1 年 LC 为 61.6%(95%CI,46.4%-73.6%),1 年 OS 为 28.5%(95%CI,19.4%-38.3%)。更高的 Karnofsky 表现状态评分(HR,0.50;95%CI,0.25-0.99;P=0.046)和在 PT-ReRT 之前接受挽救性手术(HR,0.57;95%CI,0.39-0.84;P=0.005)与 OS 改善相关,而接受四分体照射(HR,1.97;95%CI,1.36-2.86;P<0.001)与 OS 较差相关。共有 73 例 3 级和 6 例 4 级早期毒性反应。有 79 例潜在的 3 级、4 级和 5 级晚期毒性反应。
本队列研究的结果表明,与以前使用光子再放疗的报告相比,使用质子治疗再放疗的患者的生存时间更长,攻击性更强;然而,幸存的患者仍然存在早期和晚期并发症的风险。