Verberkt Carry, Lemmers Marike, de Leeuw Robert A, van Mello Norah M, Groenman Freek A, Hehenkamp Wouter J K, Huirne Judith A F
Department of Obstetrics and Gynecology, Amsterdam Reproduction and Development Research Institute, Amsterdam University Medical Center, VU Medical Center, Amsterdam, The Netherlands (Dr Verberkt).
Department of Obstetrics and Gynecology, Amsterdam University Medical Center, Amsterdam, The Netherlands (Drs Lemmers, de Leeuw, van Mello, Groenman, Hehenkamp, and Huirne).
AJOG Glob Rep. 2022 Dec 6;3(1):100143. doi: 10.1016/j.xagr.2022.100143. eCollection 2023 Feb.
There is a dramatic rise in cesarean deliveries worldwide, leading to higher complication rates in subsequent pregnancies. One of these complications is a cesarean scar pregnancy. During the last decades, treatment options for cesarean scar pregnancies have changed, and less invasive interventions have been employed to preserve fertility and reduce morbidity. However, the optimal treatment approach and the influence of various treatments on reproductive outcomes have to be determined.
This study aimed to evaluate the short- and long-term outcomes after cesarean scar pregnancy management.
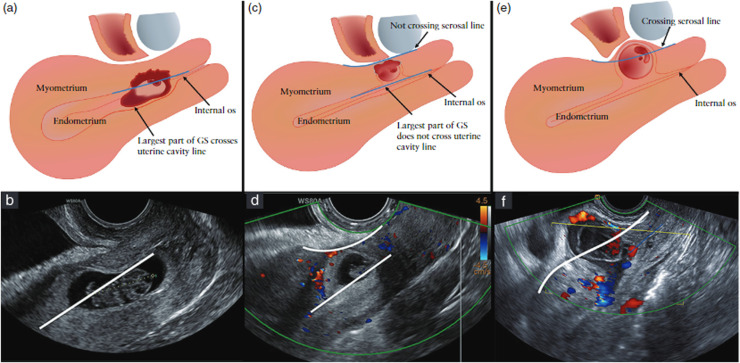
We conducted a retrospective cohort study of women determined to have a cesarean scar pregnancy from 2010 to 2021 at a tertiary referral center, the Amsterdam University Medical Center, in the Netherlands. Outcomes of the following management strategies were compared: expectant management, methotrexate, curettage with temporary cervical cerclage, or a laparoscopic niche resection. We performed a curettage if the cesarean scar pregnancy did not cross the serosal line of the uterus, and a laparoscopic niche resection was performed if the cesarean scar pregnancy crossed the serosal line. The main outcomes were treatment efficacy and time to subsequent ongoing pregnancy or pregnancy leading to a live birth.
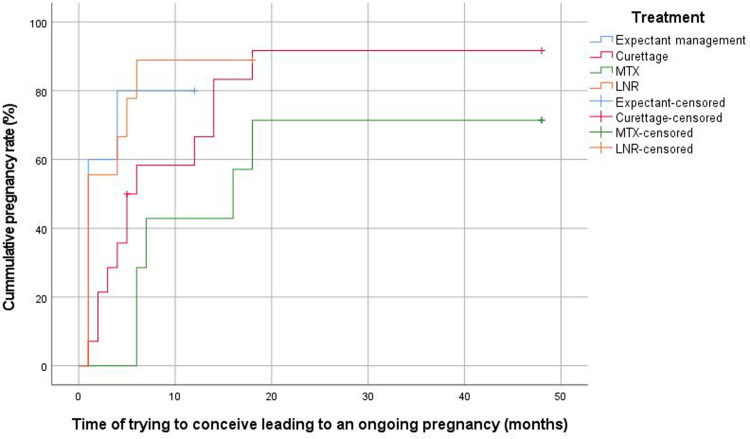
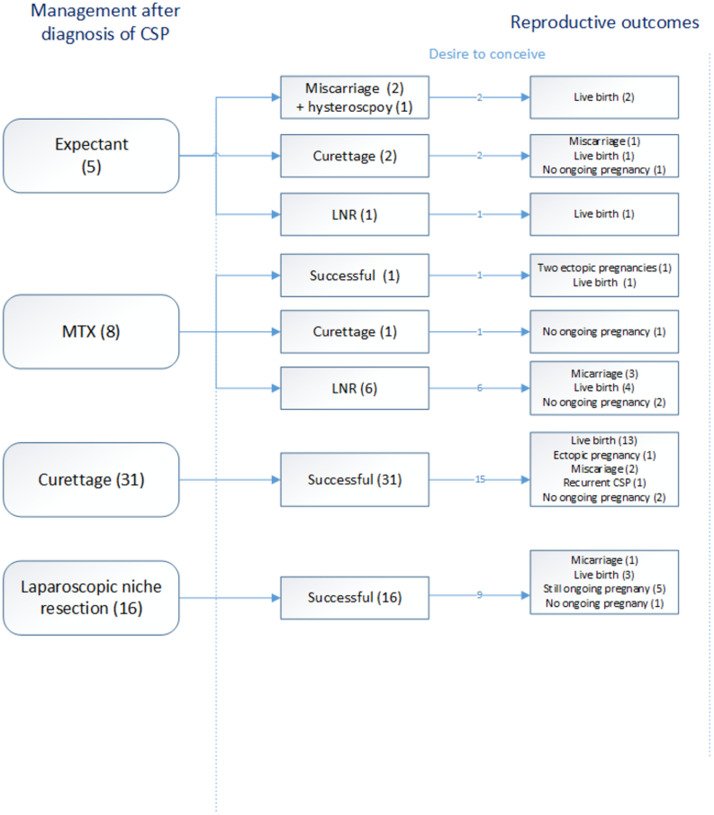
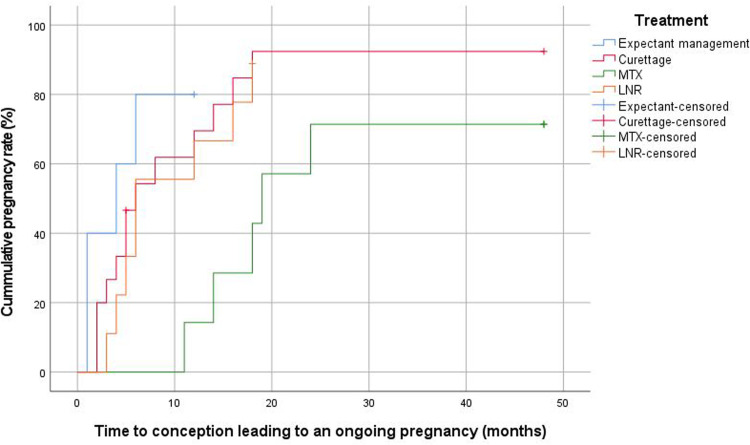
Of the 60 included women, 5 (8.3%) were managed expectantly, 8 (13.3%) were treated with methotrexate, 31 (51.8%) were treated with a curettage, and 16 (26.7%) with a laparoscopic niche resection. The groups were not comparable. The gestational age and human chorionic gonadotropin levels were generally higher in women who received methotrexate or a laparoscopic niche resection. Additional treatment in the conservative group was needed for 4 (80%) women after expectant management and for 7 (87.5%) women after methotrexate treatment. In the surgical group, all 31 women treated with a curettage and all 16 treated with a laparoscopic niche resection did not require additional treatment. The subsequent ongoing pregnancy rate after cesarean scar pregnancy management was 81.1% (30/37) among women who wished to conceive, with a live birth rate of 78.4% (29/37); 1 woman was in her third trimester of pregnancy at the time of analyses. The time between cesarean scar pregnancy management and subsequent ongoing pregnancy was 4 months (interquartile range, 3-6; =.02) after expectant management, 18 months (interquartile range, 13-22) after initial methotrexate treatment, 5 months (interquartile range, 3-14; =.01) after a curettage, and 6 months (interquartile range, 4-15; =.03) after a laparoscopic niche resection.
Surgical treatment of a cesarean scar pregnancy led to a high success rate without additional interventions, high pregnancy rates with a short time interval between treatment, and subsequent pregnancy leading to an ongoing pregnancy or live birth. Conservative management, both with expectant management and methotrexate treatment, led to high (re)intervention rates. Different management approaches are indicated for different types of cesarean scar pregnancies.
全球剖宫产率急剧上升,导致后续妊娠并发症发生率更高。其中一种并发症是剖宫产瘢痕妊娠。在过去几十年中,剖宫产瘢痕妊娠的治疗选择发生了变化,采用了侵入性较小的干预措施来保留生育能力并降低发病率。然而,最佳治疗方法以及各种治疗对生殖结局的影响仍有待确定。
本研究旨在评估剖宫产瘢痕妊娠管理后的短期和长期结局。
我们对2010年至2021年在荷兰阿姆斯特丹大学医学中心这一三级转诊中心确诊为剖宫产瘢痕妊娠的女性进行了一项回顾性队列研究。比较了以下管理策略的结局:期待治疗、甲氨蝶呤治疗、刮宫术联合临时宫颈环扎术或腹腔镜瘢痕缺损切除术。如果剖宫产瘢痕妊娠未穿过子宫浆膜层,则进行刮宫术;如果剖宫产瘢痕妊娠穿过浆膜层,则进行腹腔镜瘢痕缺损切除术。主要结局是治疗效果以及至后续持续妊娠或妊娠至活产的时间。
纳入的60名女性中,5名(8.3%)接受期待治疗,8名(13.3%)接受甲氨蝶呤治疗,31名(51.8%)接受刮宫术,16名(26.7%)接受腹腔镜瘢痕缺损切除术。各组之间不具有可比性。接受甲氨蝶呤治疗或腹腔镜瘢痕缺损切除术的女性的孕周和人绒毛膜促性腺激素水平通常较高。保守治疗组中,4名(80%)接受期待治疗的女性和7名(87.5%)接受甲氨蝶呤治疗的女性需要额外治疗。在手术组中,接受刮宫术治疗的31名女性和接受腹腔镜瘢痕缺损切除术治疗的16名女性均无需额外治疗。在希望受孕的女性中,剖宫产瘢痕妊娠管理后的后续持续妊娠率为81.1%(共37名,30名成功),活产率为78.4%(29/37);在分析时,有1名女性处于妊娠晚期。期待治疗后,剖宫产瘢痕妊娠管理至后续持续妊娠的时间为4个月(四分位间距,3 - 6;P = 0.02),初始甲氨蝶呤治疗后为18个月(四分位间距,13 - 22),刮宫术后为5个月(四分位间距,3 - 14;P = 0.01),腹腔镜瘢痕缺损切除术后为6个月(四分位间距,4 - 15;P = 0.03)。
剖宫产瘢痕妊娠的手术治疗成功率高,无需额外干预,妊娠率高,治疗后至后续妊娠的时间间隔短,且后续妊娠可发展为持续妊娠或活产。保守治疗,包括期待治疗和甲氨蝶呤治疗,导致(再次)干预率高。不同类型的剖宫产瘢痕妊娠需要不同的管理方法。