University of Michigan Department of Neurology, Ann Arbor, Michigan, USA.
Department of Child Neurology, UMC Utrecht Brain Center, Wilhelmina Children's Hospital, member of ERN EpiCare, University Medical Center Utrecht and Utrecht University, Utrecht, The Netherlands.
Epilepsia Open. 2023 Jun;8(2):371-385. doi: 10.1002/epi4.12695. Epub 2023 Feb 14.
Guidelines suggest considering antiseizure medication (ASM) discontinuation in patients with epilepsy who become seizure-free. Little is known about how discontinuation decisions are being made in practice. We measured the frequency of, and factors associated with, discussions and decisions surrounding ASM discontinuation.
We performed a multicenter retrospective cohort study at the University of Michigan (UM) and two Dutch centers: Wilhelmina Children's Hospital (WCH) and Stichting Epilepsie Instellingen Nederland (SEIN). We screened all children and adults with outpatient epilepsy visits in January 2015 and included those with at least one visit during the subsequent 2 years where they were seizure-free for at least one year. We recorded whether charts documented (1) a discussion with the patient about possible ASM discontinuation and (2) any planned attempt to discontinue at least one ASM. We conducted multilevel logistic regressions to determine factors associated with each outcome.
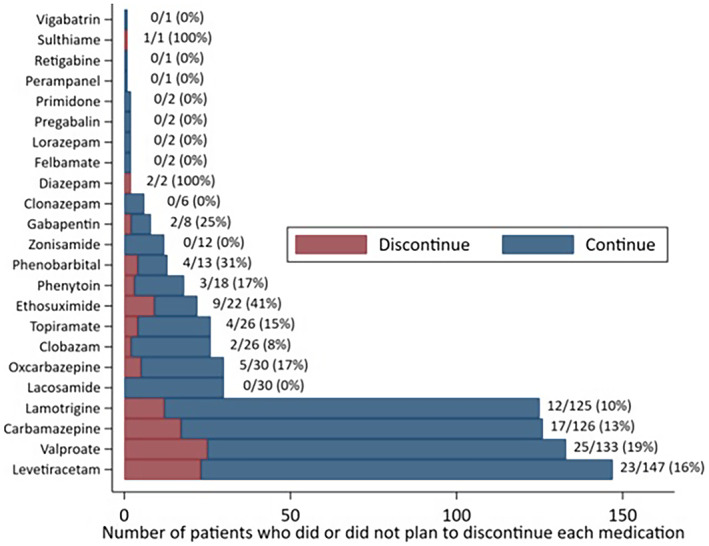
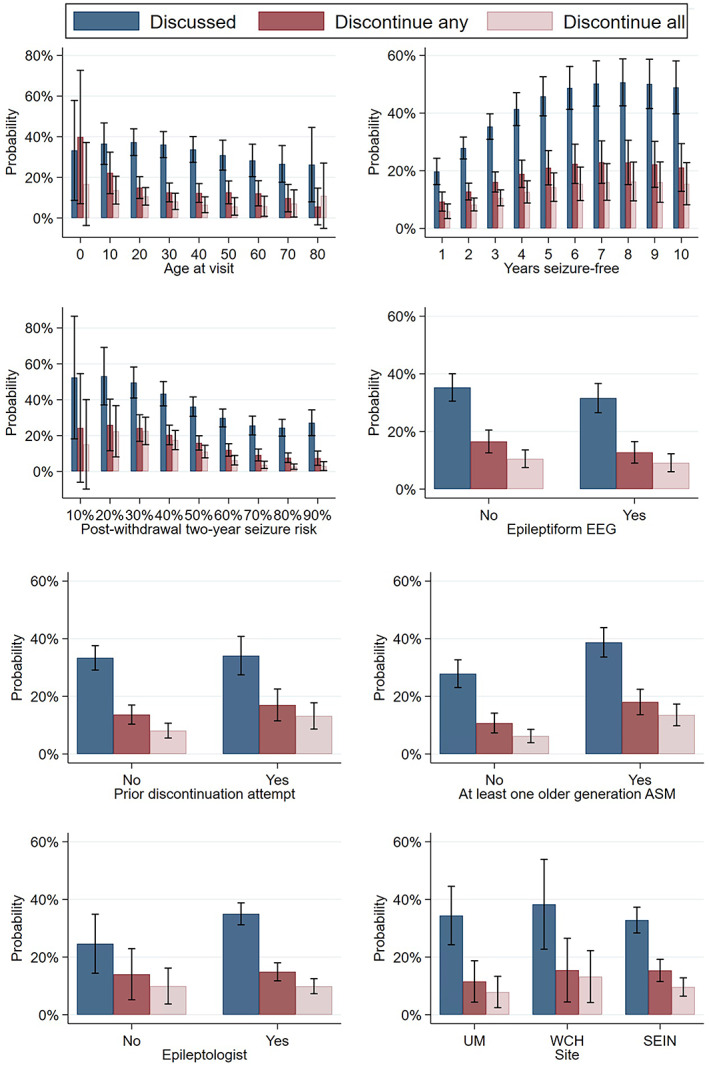
We included 1058 visits from 463 patients. Of all patients who were seizure-free at least one year, 248/463 (53%) had documentation of any discussion and 98/463 (21%) planned to discontinue at least one ASM. Corresponding frequencies for patients who were seizure-free at least 2 years were 184/285 (65%) and 74/285 (26%). The probability of discussing or discontinuing increased with longer duration of seizure freedom. Still, even for patients who were 10 years seizure-free, our models predicated that in only 49% of visits was a discontinuation discussion documented, and in only 16% of visits was it decided to discontinue all ASMs. Provider-to-provider variation explained 18% of variation in whether patients discontinued any ASM.
Only approximately half of patients with prolonged seizure freedom had a documented discussion about ASM discontinuation. Discontinuation was fairly rare even among low-risk patients. Future work should further explore barriers to and facilitators of counseling and discontinuation attempts.
指南建议在癫痫发作已得到控制的患者中考虑停止使用抗癫痫药物(ASM)。但目前对于实际操作中如何做出停药决策所知甚少。本研究旨在评估停药讨论和决策的发生频率及相关因素。
本研究在密歇根大学(UM)和荷兰的两个中心(Wilhelmina 儿童医院[WCH]和 Stichting Epilepsie Instellingen Nederland[SEIN])开展了一项多中心回顾性队列研究。我们筛选了 2015 年 1 月所有门诊癫痫就诊患者,纳入至少一次在随后 2 年内有至少 1 年无癫痫发作的就诊记录。我们记录了病历中是否记录了(1)与患者讨论停用 ASM 的可能性,以及(2)是否计划至少停用一种 ASM。我们采用多水平逻辑回归分析确定了与每个结局相关的因素。
我们纳入了 463 名患者的 1058 次就诊记录。所有至少 1 年无癫痫发作的患者中,248/463(53%)有任何讨论记录,98/463(21%)计划至少停用一种 ASM。至少 2 年无癫痫发作的患者中,对应的频率分别为 184/285(65%)和 74/285(26%)。讨论或停药的概率随癫痫无发作时间的延长而增加。然而,即使对于 10 年无癫痫发作的患者,我们的模型预测在 49%的就诊中记录了停药讨论,在 16%的就诊中决定停用所有 ASM。医生之间的差异解释了患者是否停用任何 ASM 的 18%的变异。
只有大约一半的癫痫无发作时间延长的患者有记录的关于 ASM 停药的讨论。即使是低风险患者,停药也相当罕见。未来的工作应进一步探讨咨询和停药尝试的障碍和促进因素。