Forfang Elisabeth, Larsen Kristin Tveitan, Salman Rustam Al-Shahi, Bell Simon M, Wester Per, Berge Eivind, Wyller Torgeir Bruun, Rønning Ole Morten
Institute of Clinical Medicine University of Oslo Oslo Norway.
Department of Geriatric Medicine Oslo University Hospital Oslo Norway.
Health Sci Rep. 2023 Jan 20;6(1):e1059. doi: 10.1002/hsr2.1059. eCollection 2023 Jan.
It is unclear whether patients with previous intracerebral hemorrhage (ICH) should receive antithrombotic treatment to prevent ischemic events. We assessed stroke physicians' opinions about this, and their views on randomizing patients in trials assessing this question.
We conducted three web-based surveys among stroke physicians in Scandinavia and the United Kingdom.
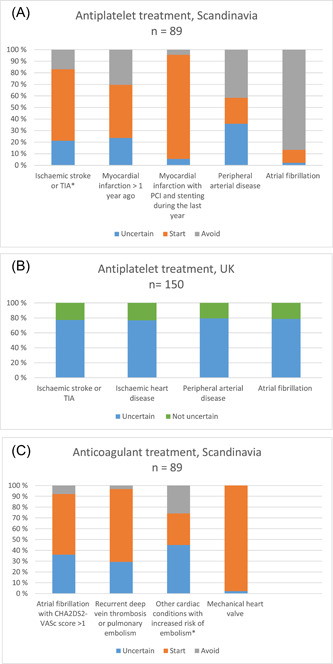
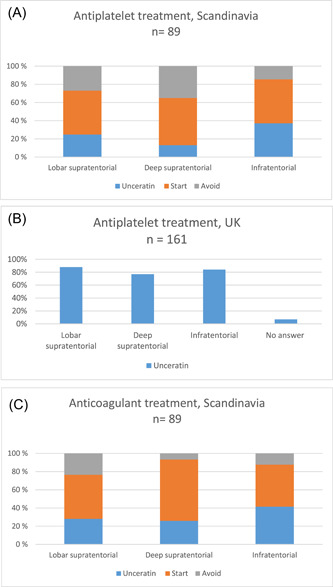
Eighty-nine of 205 stroke physicians (43%) responded to the Scandinavian survey, 161 of 180 (89%) to the UK antiplatelet survey, and 153 of 289 (53%) to the UK anticoagulant survey. In Scandinavia, 19 (21%) stroke physicians were uncertain about antiplatelet treatment after ICH for ischemic stroke or transient ischemic attack (TIA) and 21 (24%) for prior myocardial infarction. In the United Kingdom, 116 (77%) were uncertain for ischemic stroke or TIA and 115 (717%) for ischemic heart disease. In Scandinavia, 32 (36%) were uncertain about anticoagulant treatment after ICH for atrial fibrillation, and 26 (29%) for recurrent deep vein thrombosis or pulmonary embolism. In the United Kingdom, 145 (95%) were uncertain about anticoagulants after ICH in at least some cases. In both regions combined, 191 of 250 (76%) would consider randomizing ICH survivors in a trial of starting versus avoiding antiplatelets, and 176 of 242 (73%) in a trial of starting versus avoiding anticoagulants.
Considerable proportions of stroke physicians in Scandinavia and the United Kingdom were uncertain about antithrombotic treatment after ICH. A clear majority would consider randomizing patients in trials assessing this question. These findings support the need for such trials.
既往有脑出血(ICH)的患者是否应接受抗栓治疗以预防缺血性事件尚不清楚。我们评估了卒中医生对此的看法,以及他们对在评估该问题的试验中对患者进行随机分组的观点。
我们在斯堪的纳维亚半岛和英国的卒中医生中进行了三项基于网络的调查。
205名斯堪的纳维亚半岛的卒中医生中有89名(43%)回复了调查,180名英国抗血小板调查的医生中有161名(89%)回复,289名英国抗凝调查的医生中有153名(53%)回复。在斯堪的纳维亚半岛,19名(21%)卒中医生对于脑出血后抗血小板治疗预防缺血性卒中或短暂性脑缺血发作(TIA)不确定,21名(24%)对于既往心肌梗死不确定。在英国,116名(77%)对于缺血性卒中或TIA不确定,115名(717%)对于缺血性心脏病不确定。在斯堪的纳维亚半岛,32名(36%)对于脑出血后抗凝治疗预防房颤不确定,26名(29%)对于复发性深静脉血栓形成或肺栓塞不确定。在英国,145名(95%)至少在某些情况下对于脑出血后抗凝治疗不确定。在两个地区,250名医生中有191名(76%)会考虑在一项开始与避免使用抗血小板药物的试验中对脑出血幸存者进行随机分组,242名医生中有176名(73%)会考虑在一项开始与避免使用抗凝药物的试验中对脑出血幸存者进行随机分组。
斯堪的纳维亚半岛和英国相当比例的卒中医生对于脑出血后的抗栓治疗不确定。绝大多数医生会考虑在评估该问题的试验中对患者进行随机分组。这些发现支持了开展此类试验的必要性。