Chen Pang-Yen, Chen Chien-Wei, Su Yu-Jang
Department of Emergency Medicine, Mackay Memorial Hospital, Taipei 10449, Taiwan, R.O.C.
Institute of Public Health, National Yang Ming Chiao Tung University College of Medicine, Taipei 112, Taiwan, R.O.C.
Med Int (Lond). 2022 Oct 11;2(5):31. doi: 10.3892/mi.2022.56. eCollection 2022 Sep-Oct.
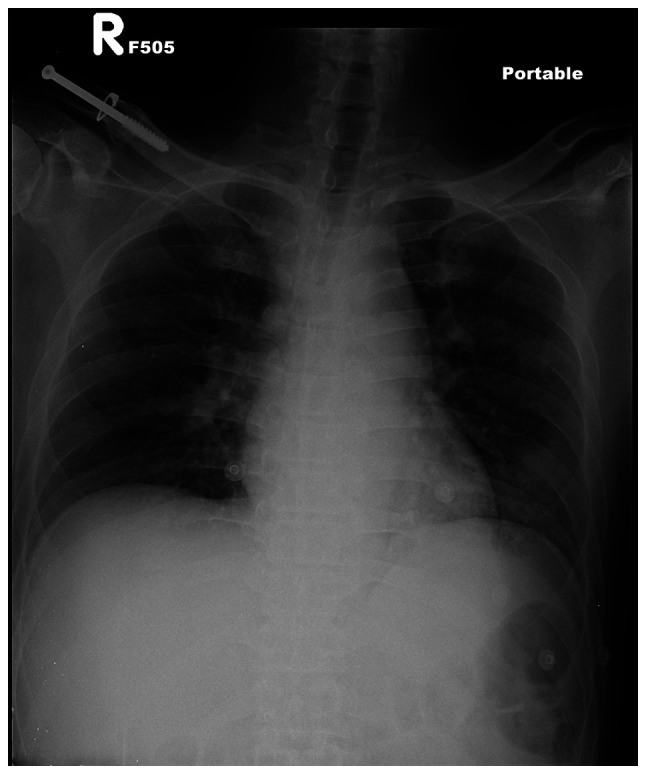
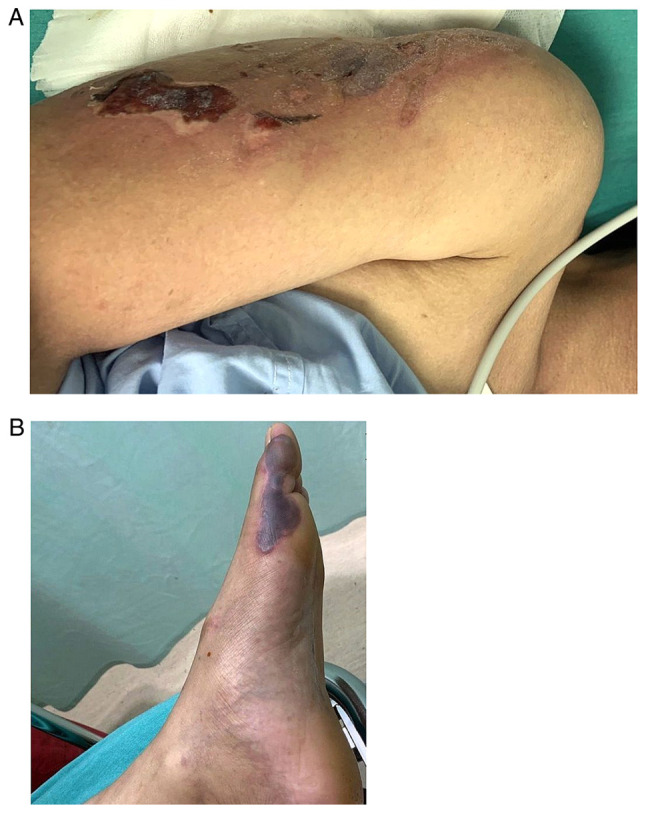
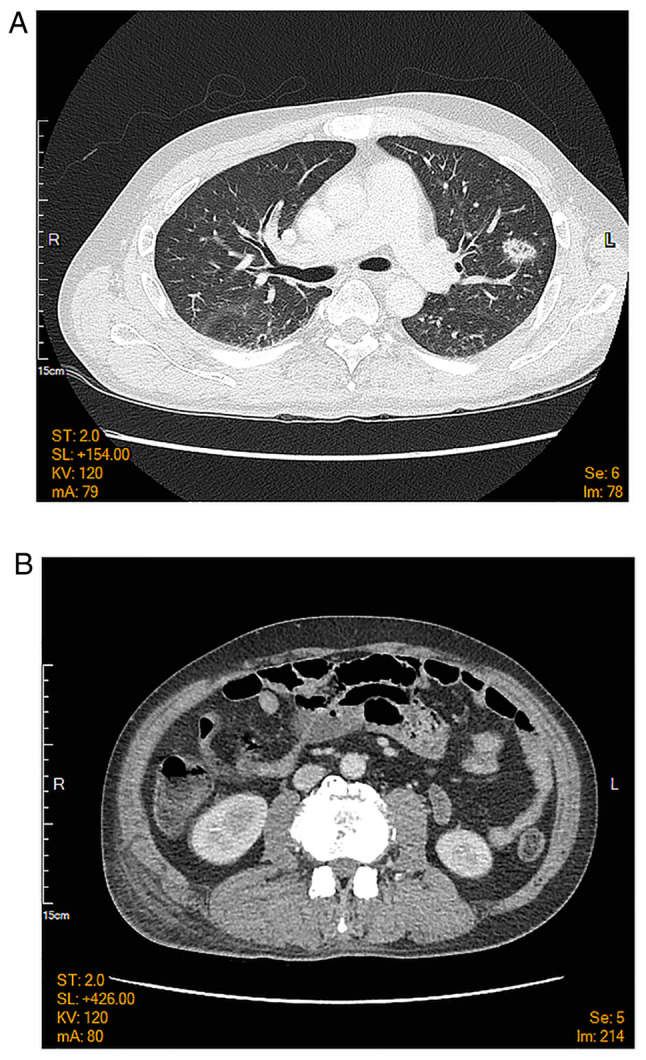
A 40-year-old male with a history of alcohol and drug addiction presented with fever for 1 day in the emergency room. He reported the abuse of drugs via intravenous injection and consumed alcohol excessively. Upon arrival to the emergency room, his body temperature was 39.4˚C. Upon a physical examination, generalized skin gangrene over the trunk and four limbs were found. Laboratory tests revealed thrombocytopenia (platelets, 67,000/µl) and elevated C-reactive protein (30.4 mg/dl), creatine kinase (>20,000 IU/l), D-Dimer (>10,000 ng/ml) levels. The urinary drug screen test was positive for ketamine and benzodiazepine. The blood culture on day 4 of admission yielded coagulase-negative (CoNS). The patient was diagnosed with CoNS induced by the venous injection of ketamine. He was admitted and received treatment with parenteral antibiotics with serial debridement due to the progressive necrosis of the skin gangrene. He was discharged 2 months later with clinical improvement. CoNS generally has a symbiotic association with the hosts in the cutaneous ecosystem, which frequently contaminates blood culture and occasionally causes diseases. CoNS should be thus considered opportunistic pathogens rather than contaminants. These organisms can cause occasional infection if the cutaneous organ system has been damaged by trauma, the direct implantation of foreign bodies or inoculation by needles. Predisposing factors for CoNS infections include an older age, immunosuppression and the implantation of medical devices, which may serve as a nidus for CoNS growth. Long-term alcoholism, drug addiction and malnutrition may have caused a decline in the immunity of the patient described herein. To date, at least to the best of our knowledge, there has been no report describing local skin necrosis induced by CoNS infection. In the case in the present study, treatment with parenteral antibiotics and serial debridement was successful. In summary, physicians need to be aware of the potential pathogenicity of CoNS in the skin and soft tissue infections.
一名有酒精和药物成瘾史的40岁男性因发热1天就诊于急诊室。他自述有静脉注射吸毒史且酗酒。到达急诊室时,他的体温为39.4˚C。体格检查发现躯干和四肢广泛性皮肤坏疽。实验室检查显示血小板减少(血小板计数67,000/µl),C反应蛋白升高(30.4mg/dl),肌酸激酶(>20,000IU/l),D-二聚体(>10,000ng/ml)水平升高。尿液药物筛查试验显示氯胺酮和苯二氮卓呈阳性。入院第4天的血培养结果为凝固酶阴性葡萄球菌(CoNS)。该患者被诊断为静脉注射氯胺酮所致的CoNS感染。由于皮肤坏疽进行性坏死,他入院后接受了肠外抗生素治疗并多次清创。2个月后他临床症状改善出院。CoNS在皮肤生态系统中通常与宿主共生,常污染血培养,偶尔致病。因此,CoNS应被视为机会致病菌而非污染物。如果皮肤器官系统因创伤、异物直接植入或针头接种而受损,这些微生物可能偶尔引起感染。CoNS感染的易感因素包括年龄较大、免疫抑制和医疗器械植入,这些可能成为CoNS生长的病灶。长期酗酒、药物成瘾和营养不良可能导致了本文所述患者免疫力下降。迄今为止,至少据我们所知,尚无CoNS感染引起局部皮肤坏死的报道。在本研究的病例中,肠外抗生素治疗和多次清创是成功的。总之,医生需要意识到CoNS在皮肤和软组织感染中的潜在致病性。