Hebei Clinical Research Center for Chronic Kidney Disease, Hebei Key Laboratory of Vascular Calcification in Kidney Disease, Department of Nephrology, The Fourth Hospital of Hebei Medical University, Shijiazhuang, P.R. China.
Medicine (Baltimore). 2023 Jan 20;102(3):e32698. doi: 10.1097/MD.0000000000032698.
Anti-glomerular basement membrane (anti-GBM) disease has been reported to coexist with other immune-mediated glomerular disorders, including antineutrophil cytoplasmic autoantibody positive glomerulonephritis and membranous glomerulopathy. It is well known that anti-GBM disease often manifests as type I crescentic glomerulonephritis on renal biopsy. However, concurrent cases of both type I crescentic glomerulonephritis and IgA nephropathy are rare.
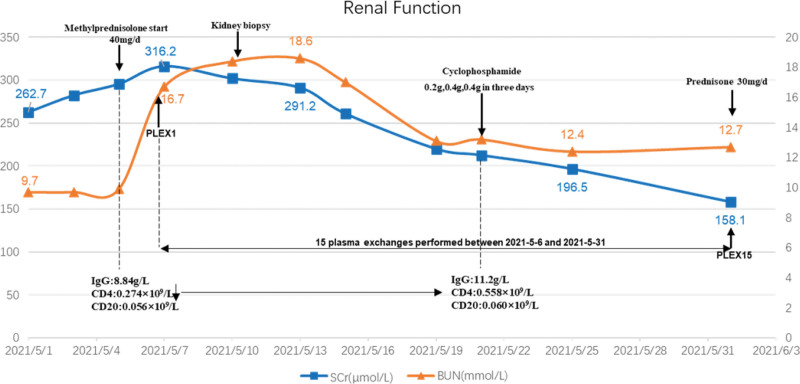
We report the case of a 40-years-old woman with microscopic hematuria, mild proteinuria and an immunocompromised status. Laboratory data revealed serum creatinine showed progressive progress, suddenly rising from the normal range to 316.2μmol/L within 4 months. The CD4 lymphocyte count was 0.274 × 109/L (reference value 0.35-1.82 × 109/L). The anti-GBM antibody titer was 192.4 IU/mL (reference range: <20 RU/mL).
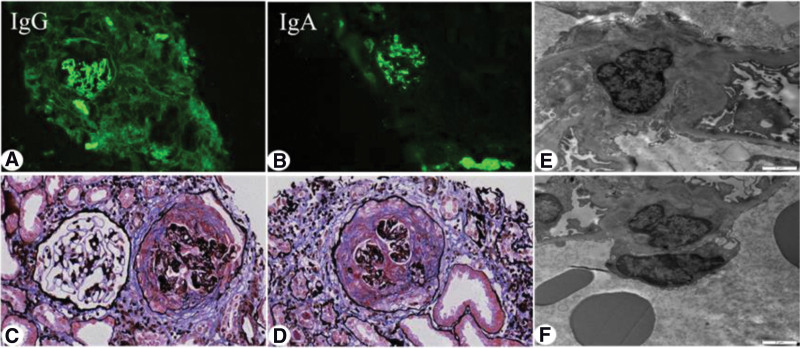
Renal biopsy was performed after admission. The pathological diagnosis was type I crescentic glomerulonephritis, IgA nephropathy, and clinical anti-GBM disease.
The patient was seriously ill on admission and progressed rapidly. Combined with poor immune function, we immediately initiated high-frequency plasma exchange (PE). In addition, to avoid rebound of antibody levels, PE was performed for 5 times. Follow-up treatment was combined with standard-dose corticosteroids and cyclophosphamide.
The patient was followed up for 1 year. On the last visit, her serum creatinine decreased to 103.5μmol/L, anti-GBM antibody remained negative, and proteinuria and hematuria disappeared.
This case illustrates that when crescentic nephritis or anti-GBM disease is combined with other immune diseases, especially when the immune function is extremely low, if the application of high-dose steroid shocks may induce fatal infections, to some extent high frequency PE has certain advantages.
抗肾小球基底膜(anti-GBM)病已被报道与其他免疫介导的肾小球疾病共存,包括中性粒细胞胞浆抗体阳性肾小球肾炎和膜性肾小球病。众所周知,抗肾小球基底膜病在肾活检时通常表现为 I 型新月体性肾小球肾炎。然而,同时存在 I 型新月体性肾小球肾炎和 IgA 肾病的情况较为罕见。
我们报告了一例 40 岁女性,表现为镜下血尿、轻度蛋白尿和免疫功能低下。实验室数据显示血清肌酐逐渐升高,在 4 个月内从正常范围突然上升至 316.2μmol/L。CD4 淋巴细胞计数为 0.274×109/L(参考值 0.35-1.82×109/L)。抗 GBM 抗体滴度为 192.4 IU/mL(参考范围:<20 RU/mL)。
入院后进行了肾活检。病理诊断为 I 型新月体性肾小球肾炎、IgA 肾病和临床抗 GBM 病。
入院时患者病情严重,进展迅速。结合免疫功能差,我们立即开始高频血浆置换(PE)。此外,为避免抗体水平反弹,共进行了 5 次 PE。后续治疗结合标准剂量皮质类固醇和环磷酰胺。
患者随访 1 年。末次随访时,血清肌酐降至 103.5μmol/L,抗 GBM 抗体阴性,蛋白尿和血尿消失。
本病例表明,当新月体性肾炎或抗 GBM 病与其他免疫性疾病合并存在,尤其是免疫功能极低时,如果应用大剂量类固醇冲击可能会诱发致命感染,在某种程度上高频 PE 具有一定优势。