Faculty of Life Sciences and Medicine, King's College London, London, United Kingdom.
Department of Clinical and Movement Neurosciences, Queen Square Institute of Neurology, University College London, London, United Kingdom.
PLoS One. 2023 Jan 27;18(1):e0259487. doi: 10.1371/journal.pone.0259487. eCollection 2023.
A diagnosis of MND takes an average 10-16 months from symptom onset. Early diagnosis is important to access supportive measures to maximise quality of life. The COVID-19 pandemic has caused significant delays in NHS pathways; the majority of GP appointments now occur online with subsequent delays in secondary care assessment. Given the rapid progression of MND, patients may be disproportionately affected resulting in late stage new presentations. We used Monte Carlo simulation to model the pre-COVID-19 diagnostic pathway and then introduced plausible COVID-19 delays.
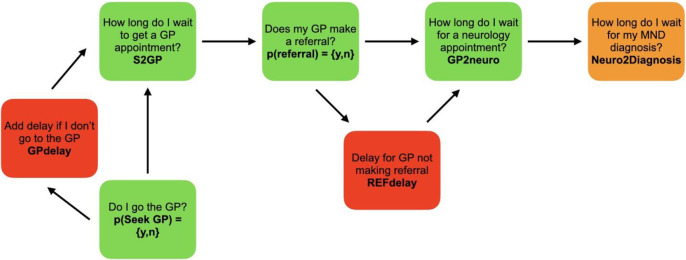
The diagnostic pathway was modelled using gamma distributions of time taken: 1) from symptom onset to GP presentation, 2) for specialist referral, and 3) for diagnosis reached after neurology appointment. We incorporated branches to simulate delays: when patients did not attend their GP and when the GP consultation did not result in referral. An emergency presentation was triggered when diagnostic pathway time was within 30 days of projected median survival. Total time-to-diagnosis was calculated over 100,000 iterations. The pre-COVID-19 model was estimated using published data and the Improving MND Care Survey 2019. We estimated COVID-19 delays using published statistics.
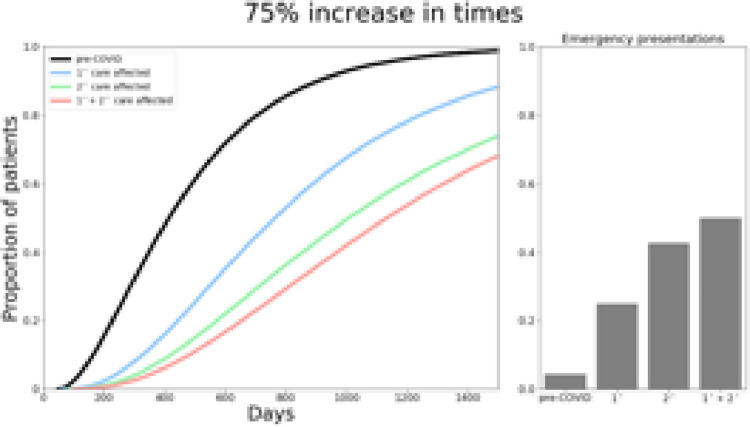
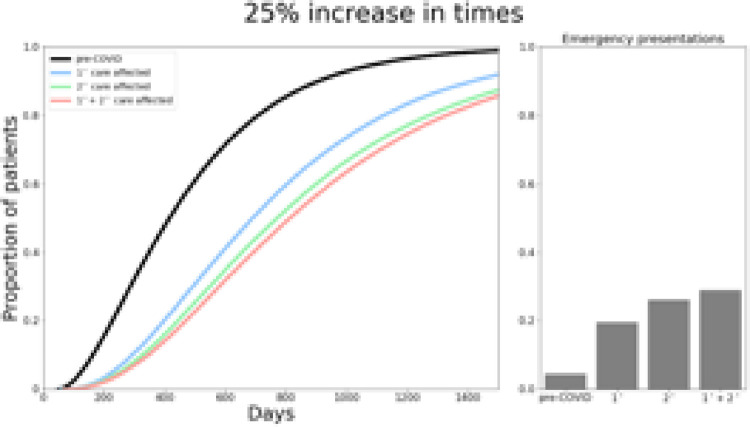
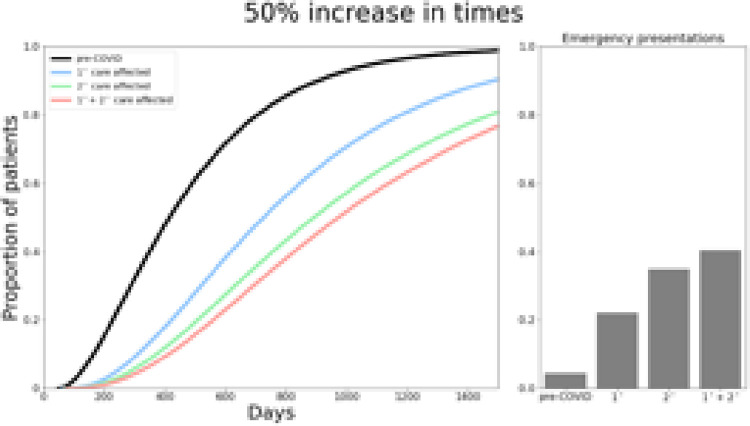
The pre-COVID model reproduced known features of the MND diagnostic pathway, with a median time to diagnosis of 399 days and predicting 5.2% of MND patients present as undiagnosed emergencies. COVID-19 resulted in diagnostic delays from 558 days when only primary care was 25% delayed, to 915 days when both primary and secondary care were 75%. The model predicted an increase in emergency presentations ranging from 15.4%-44.5%.
The model suggests the COVID-19 pandemic will result in later-stage diagnoses and more emergency presentations of undiagnosed MND. Late-stage presentations may require rapid escalation to multidisciplinary care. Proactive recognition of acute and late-stage disease with altered service provision will optimise care for people with MND.
从症状出现到确诊肌萎缩侧索硬化症(MND)平均需要 10-16 个月。早期诊断对于获得支持措施以最大限度地提高生活质量非常重要。COVID-19 大流行导致国民保健服务(NHS)路径出现了重大延误;现在大多数全科医生预约都在线进行,随后在二级保健评估中出现了延误。鉴于 MND 的快速进展,患者可能会受到不成比例的影响,导致晚期新出现的症状。我们使用蒙特卡罗模拟来模拟 COVID-19 之前的诊断路径,然后引入了合理的 COVID-19 延迟。
使用时间的伽马分布来模拟诊断途径:1)从症状出现到全科医生就诊,2)专科医生转诊,3)神经病学就诊后确诊。我们纳入了一些分支来模拟延迟:当患者未就诊和全科医生就诊后未转诊时。当诊断途径时间在预测中位生存期的 30 天内时,会触发紧急就诊。在 100,000 次迭代中计算总诊断时间。使用发表的数据和 2019 年改善 MND 护理调查对 COVID-19 之前的模型进行了估计。我们使用发表的统计数据来估计 COVID-19 延迟。
COVID-19 之前的模型再现了 MND 诊断途径的已知特征,中位诊断时间为 399 天,预测有 5.2%的 MND 患者以未确诊的紧急情况就诊。当仅初级保健延迟 25%时,COVID-19 导致诊断延迟 558 天,当初级保健和二级保健都延迟 75%时,诊断延迟 915 天。该模型预测,未确诊 MND 的紧急就诊率将增加 15.4%-44.5%。
该模型表明,COVID-19 大流行将导致更晚期的诊断和更多未确诊的 MND 紧急就诊。晚期就诊可能需要迅速升级为多学科护理。通过改变服务提供,主动识别急性和晚期疾病,将优化 MND 患者的护理。