Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA.
Broad Institute of Massachusetts Institute of Technology and Harvard University, Cambridge, MA.
Blood. 2023 Apr 13;141(15):1817-1830. doi: 10.1182/blood.2022018246.
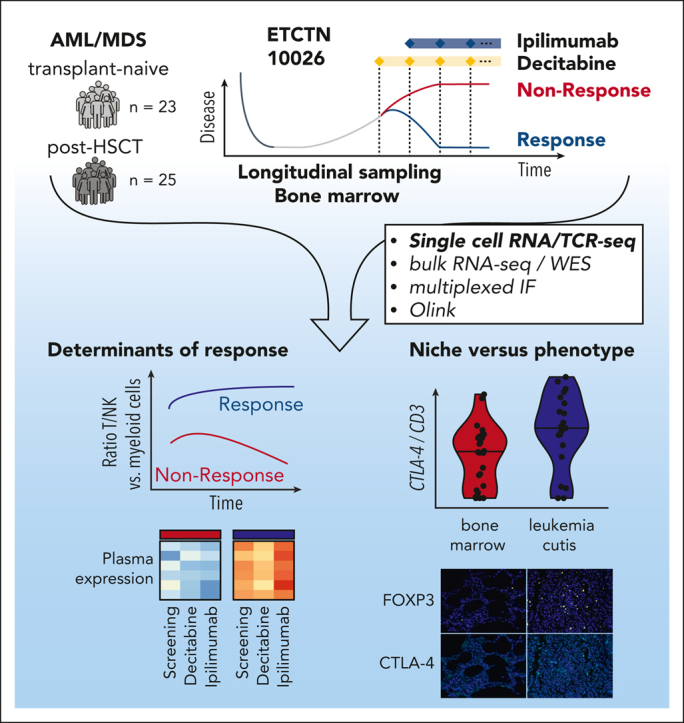
The challenge of eradicating leukemia in patients with acute myelogenous leukemia (AML) after initial cytoreduction has motivated modern efforts to combine synergistic active modalities including immunotherapy. Recently, the ETCTN/CTEP 10026 study tested the combination of the DNA methyltransferase inhibitor decitabine together with the immune checkpoint inhibitor ipilimumab for AML/myelodysplastic syndrome (MDS) either after allogeneic hematopoietic stem cell transplantation (HSCT) or in the HSCT-naïve setting. Integrative transcriptome-based analysis of 304 961 individual marrow-infiltrating cells for 18 of 48 subjects treated on study revealed the strong association of response with a high baseline ratio of T to AML cells. Clinical responses were predominantly driven by decitabine-induced cytoreduction. Evidence of immune activation was only apparent after ipilimumab exposure, which altered CD4+ T-cell gene expression, in line with ongoing T-cell differentiation and increased frequency of marrow-infiltrating regulatory T cells. For post-HSCT samples, relapse could be attributed to insufficient clearing of malignant clones in progenitor cell populations. In contrast to AML/MDS bone marrow, the transcriptomes of leukemia cutis samples from patients with durable remission after ipilimumab monotherapy showed evidence of increased infiltration with antigen-experienced resident memory T cells and higher expression of CTLA-4 and FOXP3. Altogether, activity of combined decitabine and ipilimumab is impacted by cellular expression states within the microenvironmental niche of leukemic cells. The inadequate elimination of leukemic progenitors mandates urgent development of novel approaches for targeting these cell populations to generate long-lasting responses. This trial was registered at www.clinicaltrials.gov as #NCT02890329.
消除经过初始细胞减灭治疗后的急性髓系白血病(AML)患者中的白血病这一挑战,促使现代努力将包括免疫疗法在内的协同有效方式相结合。最近,ETCTN/CTEP 10026 研究测试了 DNA 甲基转移酶抑制剂地西他滨与免疫检查点抑制剂伊匹单抗联合用于 AML/骨髓增生异常综合征(MDS)的治疗,这些患者或接受了异基因造血干细胞移植(HSCT),或在未接受 HSCT 的情况下接受治疗。对 48 例接受研究治疗的患者中的 18 例患者的 304961 个骨髓浸润细胞的综合转录组分析表明,反应与 T 细胞与 AML 细胞的基线高比例强烈相关。临床反应主要由地西他滨诱导的细胞减少驱动。只有在接受伊匹单抗暴露后才会出现免疫激活的证据,这改变了 CD4+T 细胞的基因表达,与正在进行的 T 细胞分化和骨髓浸润调节性 T 细胞的频率增加一致。对于 HSCT 后样本,复发可归因于祖细胞群体中恶性克隆清除不足。与 AML/MDS 骨髓相比,接受伊匹单抗单药治疗后持久缓解的白血病皮肤样本的转录组显示出抗原经验驻留记忆 T 细胞浸润增加和 CTLA-4 和 FOXP3 表达增加的证据。总的来说,联合地西他滨和伊匹单抗的活性受到白血病细胞微环境龛内细胞表达状态的影响。白血病祖细胞的清除不足,迫切需要开发针对这些细胞群体的新方法来产生持久的反应。该试验在 www.clinicaltrials.gov 上注册为 #NCT02890329。