Cardiology Service, Department of Medicine, Walter Reed National Military Medical Center, Bethesda, Maryland, USA.
Cardiology Service, Department of Medicine, Brooke Army Medical Center, San Antonio, Texas, USA
Open Heart. 2023 Jan;10(1). doi: 10.1136/openhrt-2022-002093.
ST elevation myocardial infarction (STEMI) represents a cardiac emergency. Time to diagnosis, identification of culprit lesion, and intervention are important. Inferior STEMI represents a dilemma for cardiologists. The territory can be supplied by the right coronary artery (RCA) or the left circumflex coronary artery (LCx). Diagnostic algorithms have been proposed to predict the culprit artery.
We performed a single-centre retrospective cohort analysis of all patients admitted to our hospital from 2008 to 2020 with a diagnosis of inferior STEMI. We examined the diagnostic 12 lead ECG for quantification of ST elevation in leads II and III and compared this to culprit lesion found on angiography.
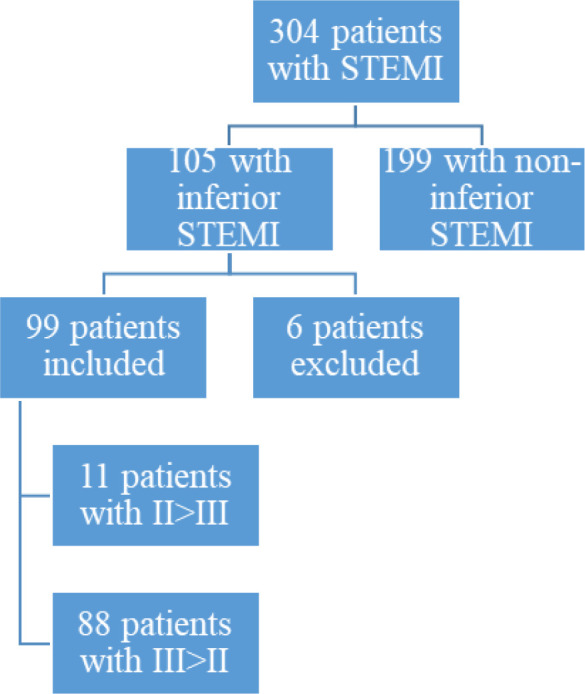
There were 304 patients identified with STEMI in our database; 105 were found to have an inferior myocardial infarction by ECG criteria. Ninety-nine were included in our study with either RCA or LCx culprit lesions on angiography (82 males, 17 females). The average age of these patients was 64.9 years old. Sensitivity, specificity, positive predictive value and negative predictive value for ST elevation in lead II exceeding lead III predicting LCx culprit lesion was 0.32 (95% CI 0.13 to 0.57), 0.94 (95% CI 0.86 to 0.98), 0.55 (95% CI 0.29 to 0.78), 0.85 (95% CI 0.81 to 0.89), respectively. Sensitivity, specificity, positive predictive value and negative predictive value for ST elevation in lead III exceeding lead II predicting RCA culprit lesion was 0.94 (95% CI 0.86 to 0.98), 0.32 (95% CI 0.13 to 0.57), 0.85 (95% CI 0.81 to 0.89), 0.55 (95% CI 0.29 to 0.78), respectively.
In inferior STEMI, comparison of ST elevation in leads II and III can reliably predict culprit lesion artery and guide intervention.
Culprit artery localisation, inferior stemi, ECG.
ST 段抬高型心肌梗死(STEMI)代表一种心脏急症。诊断时间、罪犯病变的识别和干预都很重要。下壁 STEMI 对心脏病专家来说是一个困境。该区域可由右冠状动脉(RCA)或左回旋支冠状动脉(LCx)供应。已经提出了一些诊断算法来预测罪犯动脉。
我们对 2008 年至 2020 年期间因诊断为下壁 STEMI 而入住我院的所有患者进行了单中心回顾性队列分析。我们检查了 12 导联心电图以量化 II 导联和 III 导联的 ST 段抬高,并将其与血管造影发现的罪犯病变进行比较。
我们的数据库中确定了 304 例 STEMI 患者;105 例心电图标准下诊断为下壁心肌梗死。99 例患者纳入本研究,血管造影显示 RCA 或 LCx 有罪犯病变(82 例男性,17 例女性)。这些患者的平均年龄为 64.9 岁。ST 段抬高在 II 导联超过 III 导联预测 LCx 罪犯病变的敏感性、特异性、阳性预测值和阴性预测值分别为 0.32(95%CI 0.13 至 0.57)、0.94(95%CI 0.86 至 0.98)、0.55(95%CI 0.29 至 0.78)、0.85(95%CI 0.81 至 0.89)。ST 段抬高在 III 导联超过 II 导联预测 RCA 罪犯病变的敏感性、特异性、阳性预测值和阴性预测值分别为 0.94(95%CI 0.86 至 0.98)、0.32(95%CI 0.13 至 0.57)、0.85(95%CI 0.81 至 0.89)、0.55(95%CI 0.29 至 0.78)。
在下壁 STEMI 中,比较 II 导联和 III 导联的 ST 段抬高可以可靠地预测罪犯病变动脉并指导干预。
罪犯动脉定位,下壁 ST 段抬高,心电图。