McNair Adina, Melmer Patrick D, Pinnola Aaron D
General Surgery, Grand Strand Medical Center, Myrtle Beach, USA.
Acute Care Surgery, Virginia Commonwealth University, Richmond, USA.
Cureus. 2022 Dec 26;14(12):e32965. doi: 10.7759/cureus.32965. eCollection 2022 Dec.
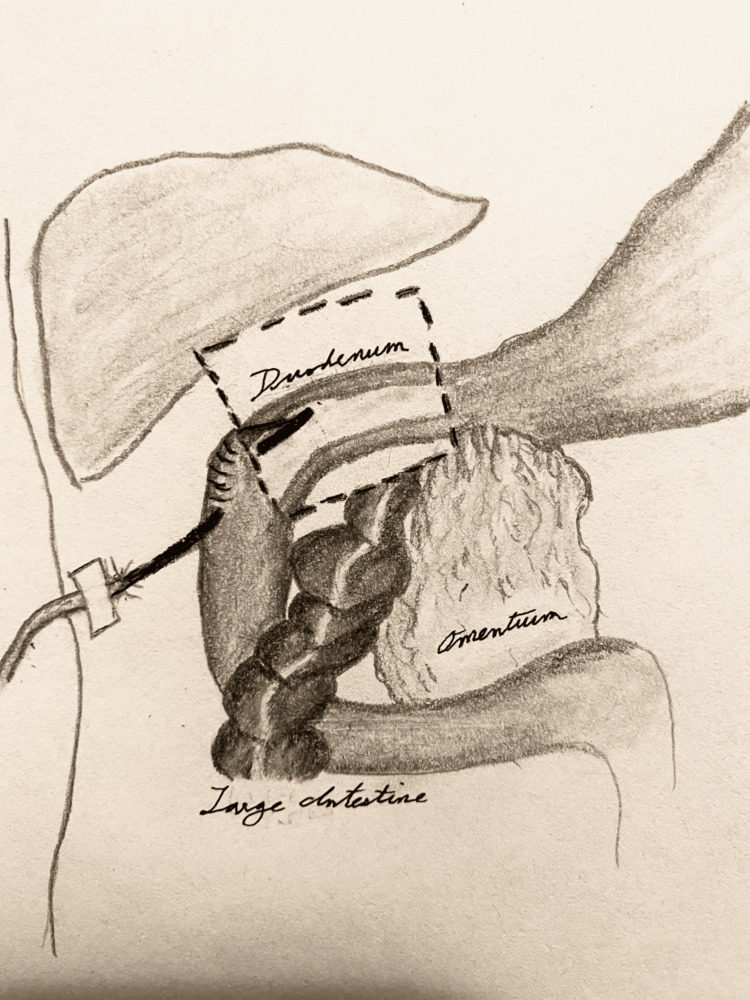
Tube duodenostomy has been described as a useful technique in the management of difficult duodenum arising from a variety of pathologies. In addition, the use of a t-tube for the duodenostomy presents a resourceful option in the event of Malecot or other such catheter unavailability. The aim of our study is to describe the technique and outcomes associated with this approach. During a six-month period in 2020, t-tube duodenostomies were performed in three patients for duodenal stump perforation: the first case involved a patient with Roux-en-Y esophagojejunostomy anatomy; the second involved duodenal stump closure security following Billroth II gastrectomy for peptic ulcer disease; and the third involved decompression following primary closure of duodenal perforation. All duodenostomies were performed with a t-tube that was trimmed with the back wall divided and then secured via the Witzel approach. The t-tube duodenostomies were performed during the index operations of all patients. No patient required additional operations. There was no mortality. All patients were closely monitored postoperatively with duodenostomies kept in place for six weeks. One patient developed a small leak after a trial of tube clamping, which was managed with continued tube drainage and antibiotics prior to definitive removal. The mean length of stay was 20.3 days with two patients being discharged to rehab. T-tube duodenostomy is a simple technique that helps avoid the blowout of the vulnerable duodenal stump in situations of biliopancreatic limb pathology, ulcerative disease, or injury.
十二指肠造瘘术已被描述为一种用于处理由多种病理状况引起的复杂十二指肠问题的有用技术。此外,在无法获得马勒科特导管或其他此类导管的情况下,使用T型管进行十二指肠造瘘术是一种明智的选择。我们研究的目的是描述这种方法的技术及相关结果。在2020年的六个月期间,对三名患者进行了T型管十二指肠造瘘术以处理十二指肠残端穿孔:第一例患者具有 Roux-en-Y 食管空肠吻合术解剖结构;第二例涉及因消化性溃疡疾病行毕罗Ⅱ式胃切除术后十二指肠残端闭合的安全性;第三例涉及十二指肠穿孔一期缝合后的减压。所有十二指肠造瘘术均使用修剪过的T型管,其后壁分开,然后通过维泽尔方法固定。T型管十二指肠造瘘术在所有患者的初次手术期间进行。没有患者需要额外的手术。没有死亡病例。所有患者术后均密切监测,十二指肠造瘘管保留六周。一名患者在试行夹管后出现小渗漏,在最终拔除之前通过持续的管腔引流和使用抗生素进行处理。平均住院时间为20.3天,两名患者出院后前往康复机构。T型管十二指肠造瘘术是一种简单的技术,有助于避免在胆胰肢体病变、溃疡性疾病或损伤情况下脆弱的十二指肠残端破裂。