Ding Li, Deng Xiaobin, Wang Kun, Xia Wentao, Zhang Yang, Zhang Yan, Shao Xianfeng, Wang Junqi
Department of Urology, the Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, 221000, People's Republic of China.
Department of Urology, the First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi Zhuang Autonomous Region, 530000, People's Republic of China.
J Inflamm Res. 2023 Jan 21;16:283-296. doi: 10.2147/JIR.S393511. eCollection 2023.
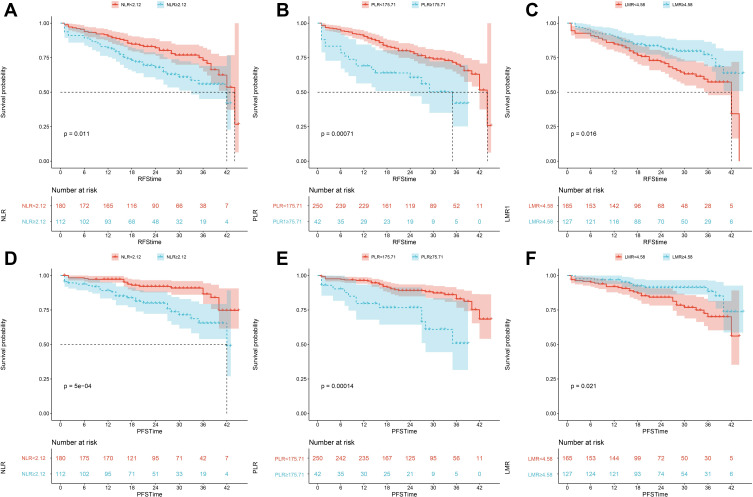
Neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), and lymphocyte/monocyte ratio (LMR) have been widely proposed to have predictive value for the patient prognosis of many malignancies, including bladder cancer. However, the predictive value of their combination in non-muscle-invasive bladder cancer (NMIBC) is unclear.
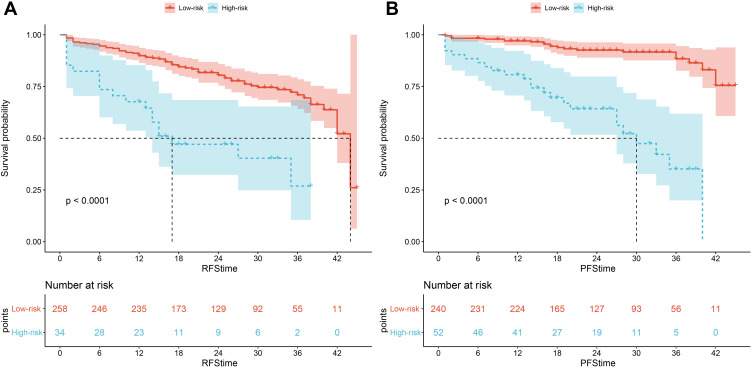
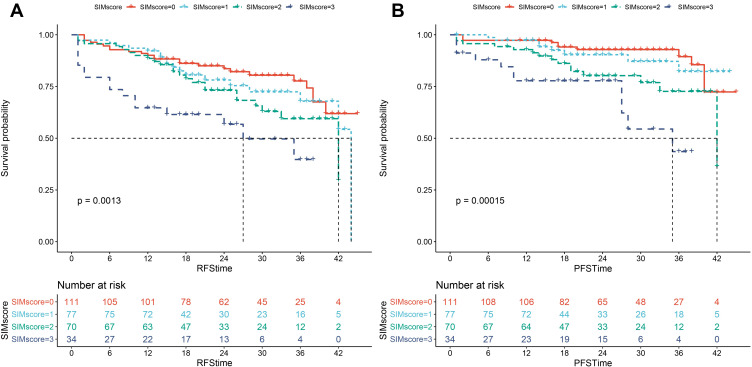
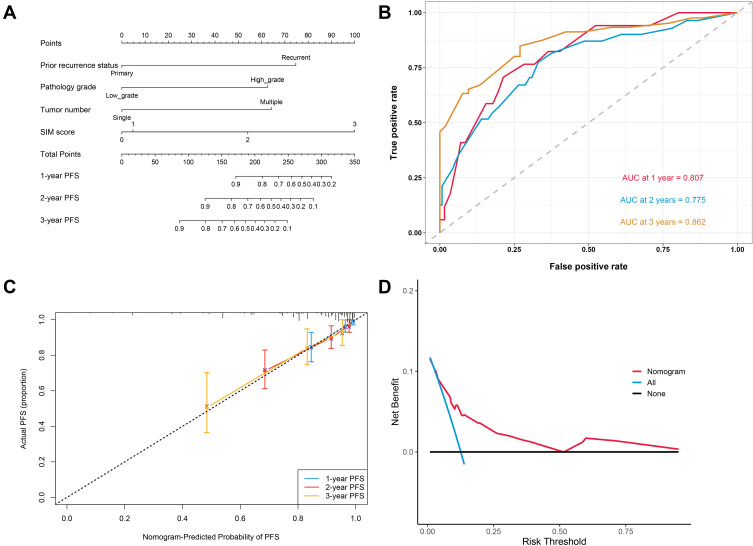
Cases of NMIBC patients who underwent transurethral resection of the bladder tumor were recruited from two tertiary public medical centers. A systemic inflammatory marker (SIM) score was calculated based on comprehensive consideration of NLR, PLR, and LMR. Recurrence-free survival (RFS) and progression-free survival (PFS) were estimated by Kaplan-Meier analysis. The Log rank test was used to compare differences between the groups. Cox regression was used to screen risk factors affecting RFS and PFS. Nomogram models were established and validated, and patients were stratified based on the model scores.
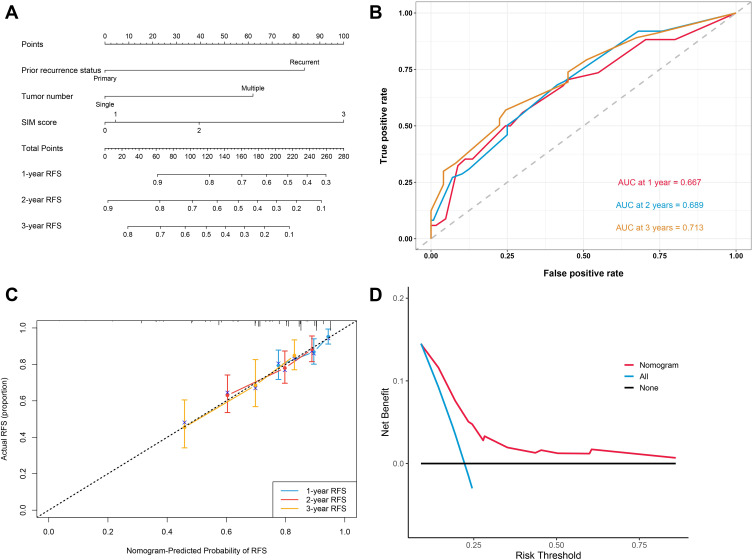
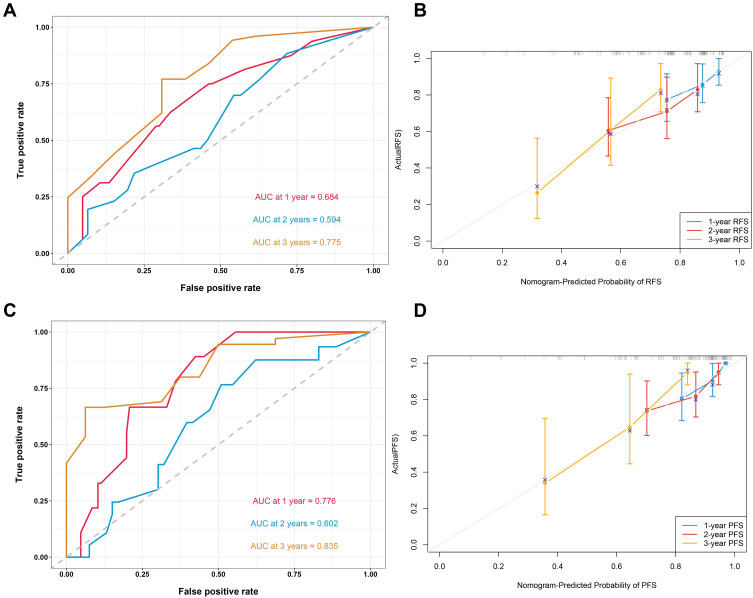
The study dataset was grouped according to a 7:3 randomization, with the training cohort consisting of 292 cases and the validation cohort consisting of 124 cases. Cox regression analysis showed that SIM score is an independent predictor of RFS and PFS in NMIBC patients. The novel models were established based on the SIM score and other statistically significant clinicopathological features. The area under the curve (AUC) for predicting 1-, 2-, and 3-year RFS was 0.667, 0.689, and 0.713, respectively. The AUC for predicting 1-, 2-, and 3-year PFS was 0.807, 0.775, and 0.862, respectively. Based on the risk stratification, patients at high risk of recurrence and progression could be accurately identified. The established models were applied to the patient evaluation of the validation cohort, which proved the great performance of the novel models.
The novel models based on the SIM score and clinicopathological characteristics can accurately predict the survival prognosis of NMIBC patients, and the models can be used by clinicians for individualized patient assessment and to assist in clinical decision-making.
中性粒细胞/淋巴细胞比值(NLR)、血小板/淋巴细胞比值(PLR)和淋巴细胞/单核细胞比值(LMR)已被广泛认为对包括膀胱癌在内的多种恶性肿瘤患者的预后具有预测价值。然而,它们的联合在非肌层浸润性膀胱癌(NMIBC)中的预测价值尚不清楚。
从两家三级公立医疗中心招募接受经尿道膀胱肿瘤切除术的NMIBC患者。基于对NLR、PLR和LMR的综合考虑计算全身炎症标志物(SIM)评分。采用Kaplan-Meier分析估计无复发生存期(RFS)和无进展生存期(PFS)。采用对数秩检验比较组间差异。采用Cox回归筛选影响RFS和PFS的危险因素。建立并验证列线图模型,并根据模型评分对患者进行分层。
研究数据集按7:3随机分组,训练队列包括292例患者,验证队列包括124例患者。Cox回归分析表明,SIM评分是NMIBC患者RFS和PFS的独立预测因子。基于SIM评分和其他具有统计学意义的临床病理特征建立了新模型。预测1年、2年和3年RFS的曲线下面积(AUC)分别为0.667、0.689和0.713。预测1年、2年和3年PFS的AUC分别为0.807、0.775和0.862。基于风险分层,可以准确识别复发和进展高危患者。将建立的模型应用于验证队列的患者评估,证明了新模型的良好性能。
基于SIM评分和临床病理特征的新模型可以准确预测NMIBC患者的生存预后,临床医生可以使用这些模型进行个体化患者评估,并协助临床决策。