Liu Weidong, Kong Wenjie, Hui Wenjia, Wang Chun, Jiang Qi, Shi Hong, Gao Feng
College of Life Science and Technology, Xinjiang University, Urumqi, China.
Department of Gastroenterology, People's Hospital of Xinjiang Uygur Autonomous Region, Urumqi, China.
Front Microbiol. 2023 Jan 13;13:999564. doi: 10.3389/fmicb.2022.999564. eCollection 2022.
Different types of were analyzed to determine their infection characteristics using serology, pathology, and non-magnification white light endoscopy combined with the Kimura-Takemoto classification, and the regular arrangement of collecting venules (RAC) as well.
A retrospective analysis of 685 inpatients who have completed the C-urea breath test, the antibody typing classification, the serum gastric function tests (PGI/PGII/G-17), the endoscope detection, and the pathological examinations.
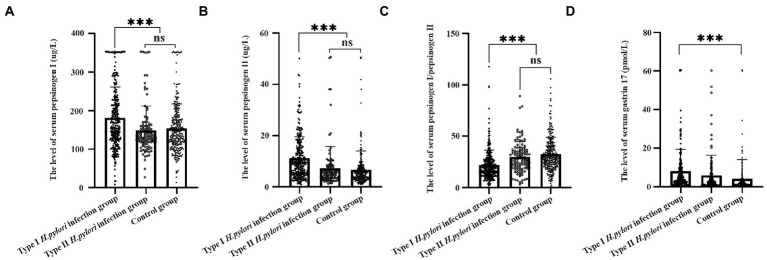
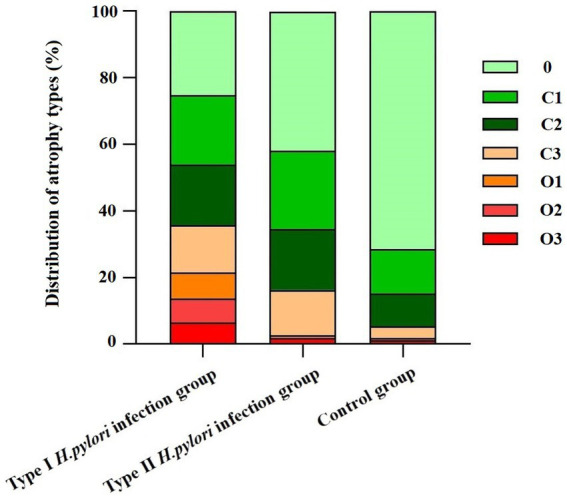
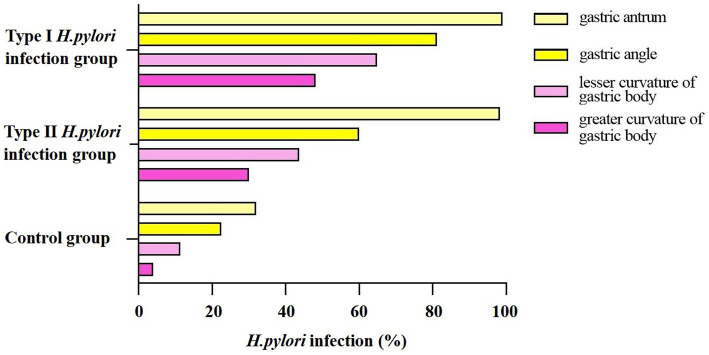
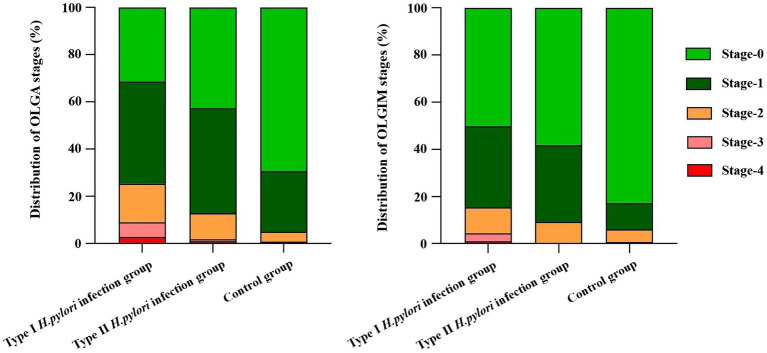
The levels of PGI, PGII, and G-17 were in descending order from the type I infection group to the type II infection group than the control group ( = 14.31; 26.23; 9.12, < 0.01). Using the Kimura-Takemoto classification, there were significant differences among the three groups of different degrees of atrophy ( =29.81; 482.78; 292.5, 0.01). Based on the characteristics of RAC, the infection rates were in descending order from the type I infection group to the type II infection group than the control group ( = 200.39; 174.72; 143.51, < 0.01). The type I infection group had higher grades than those of the type II infection group in the OLGA and OLGIM staging systems, while the differences are statistically significant only in the OLGA staging system ( =10.63, < 0.05).
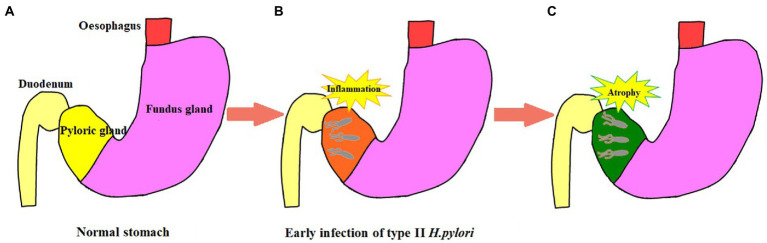
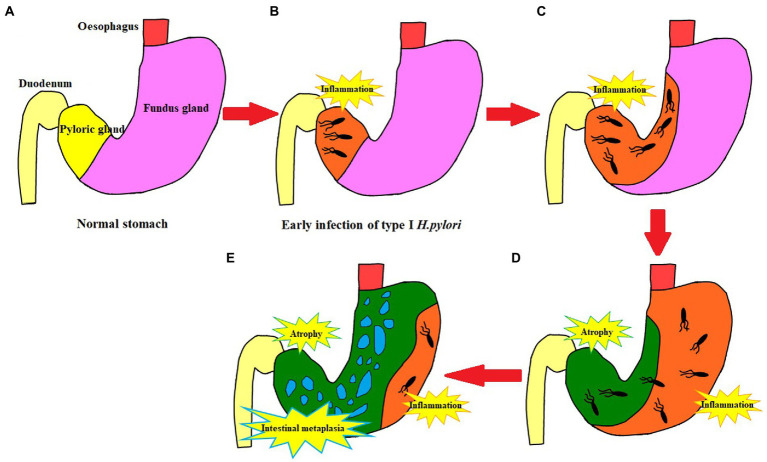
With the aid of non-amplified white light endoscopy, we found new evidence of type I infection accelerating the progression of gastric mucosal atrophy through the degree of atrophy and the range of infection, whereas type II infection has a low ability of migration and atrophy progression. Individual virulence factor-based eradication therapy may be a better choice in future.
采用血清学、病理学以及非放大白光内镜结合木村 - 竹本分类法,对不同类型的[未提及具体病原体,原文此处表述有误]进行分析,以确定其感染特征,同时也分析了集合小静脉的规则排列(RAC)情况。
对685例已完成碳 - 尿素呼气试验、[未提及具体抗体,原文此处表述有误]抗体分型分类、血清胃功能检测(PGI/PGII/G - 17)、内镜检测及病理检查的住院患者进行回顾性分析。
从Ⅰ型[未提及具体病原体,原文此处表述有误]感染组到Ⅱ型[未提及具体病原体,原文此处表述有误]感染组,PGI、PGII和G - 17水平较对照组呈下降趋势(F = 14.31;26.23;9.12,P < 0.01)。采用木村 - 竹本分类法,不同程度萎缩的三组之间存在显著差异(F = 29.81;482.78;292.5,P < 0.01)。基于RAC特征,从Ⅰ型[未提及具体病原体,原文此处表述有误]感染组到Ⅱ型[未提及具体病原体,原文此处表述有误]感染组,[未提及具体病原体,原文此处表述有误]感染率较对照组呈下降趋势(F = 200.39;174.72;143.51,P < 0.01)。在OLGA和OLGIM分期系统中,Ⅰ型[未提及具体病原体,原文此处表述有误]感染组的分期高于Ⅱ型[未提及具体病原体,原文此处表述有误]感染组,而仅在OLGA分期系统中差异具有统计学意义(F = 10.63,P < 0.05)。
借助非放大白光内镜,我们发现了新的证据,即Ⅰ型[未提及具体病原体,原文此处表述有误]感染通过萎缩程度和感染范围加速胃黏膜萎缩的进展,而Ⅱ型[未提及具体病原体,原文此处表述有误]感染的迁移和萎缩进展能力较低。未来基于个体毒力因子的根除治疗可能是更好的选择。