Division of Global Health Equity, Department of Medicine, Brigham and Women's Hospital, 75 Francis St, Boston, MA, USA.
Program in Global Noncommunicable Disease and Social Change, Department of Global Health and Social Medicine, Harvard Medical School, 641 Huntington Ave, Boston, MA, USA.
BMC Health Serv Res. 2023 Jan 30;23(1):99. doi: 10.1186/s12913-023-09072-9.
Noncommunicable diseases (NCDs) and mental health conditions represent a growing proportion of disease burden in low- and middle-income countries (LMICs). While past efforts have identified interventions to be delivered across health system levels to address this burden, the challenge remains of how to deliver heterogenous interventions in resource-constrained settings. One possible solution is the Integration of interventions within existing care delivery models. This study reviews and summarizes published literature on models of integrated NCD and mental health care in LMICs.
We searched Pubmed, African Index Medicus and reference lists to conduct a scoping review of studies describing an integrated model of NCD or neuropsychiatric conditions (NPs) implemented in a LMIC. Conditions of interest were grouped into common and severe NCDs and NPs. We identified domains of interest and types of service integration, conducting a narrative synthesis of study types. Studies were screened and characteristics were extracted for all relevant studies. Results are reported using PRISMA-ScR.
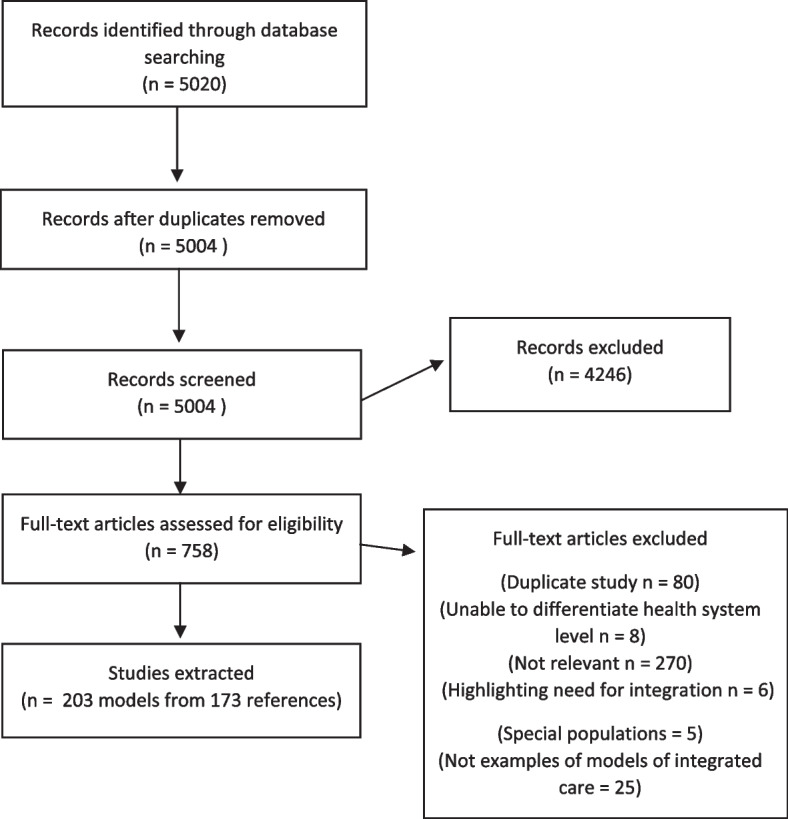
Our search yielded 5004 studies, we included 219 models of integration from 188 studies. Most studies were conducted in middle-income countries, with the majority in sub-Saharan Africa. Health services were offered across all health system levels, with most models implemented at health centers. Common NCDs (including type 2 diabetes and hypertension) were most frequently addressed by these models, followed by common NPs (including depression and anxiety). Conditions and/or services were often integrated into existing primary healthcare, HIV, maternal and child health programs. Services provided for conditions of interest varied and frequency of these services differed across health system levels. Many models demonstrated decentralization of services to lower health system levels, and task shifting to lower cadre providers.
While integrated service design is a promising method to achieve ambitious global goals, little is known about what works, when, and why. This review characterizing care integration programs is an initial step toward developing a structured study of care integration.
在中低收入国家(LMICs),非传染性疾病(NCDs)和精神健康状况占疾病负担的比例不断增加。虽然过去的努力已经确定了需要在整个卫生系统层面上实施的干预措施来解决这一负担,但在资源有限的环境下实施异质干预措施仍然是一个挑战。一个可能的解决方案是将干预措施纳入现有的医疗服务模式中。本研究综述并总结了在 LMICs 中实施的综合 NCD 和精神卫生保健模式的已发表文献。
我们在 Pubmed、非洲医学索引和参考文献中进行了检索,以对描述在 LMICs 中实施的 NCD 或神经精神疾病(NPs)综合模式的研究进行范围界定审查。有兴趣的疾病被分为常见和严重的 NCDs 和 NPs。我们确定了感兴趣的领域和服务整合类型,对研究类型进行了叙述性综合。对所有相关研究进行了筛选,并提取了研究特征。结果使用 PRISMA-ScR 报告。
我们的搜索产生了 5004 项研究,我们从 188 项研究中纳入了 219 个整合模式。大多数研究是在中等收入国家进行的,其中大部分在撒哈拉以南非洲。卫生服务在所有卫生系统层面都有提供,大多数模式在卫生中心实施。这些模式最常针对常见的 NCD(包括 2 型糖尿病和高血压),其次是常见的 NPs(包括抑郁和焦虑)。条件和/或服务经常被整合到现有的初级保健、艾滋病毒、母婴健康计划中。为感兴趣的疾病提供的服务各不相同,这些服务在卫生系统层面上的频率也不同。许多模式都展示了服务向较低卫生系统层面的去中心化,以及向低级别医务人员的任务转移。
虽然综合服务设计是实现雄心勃勃的全球目标的一种有前途的方法,但对于什么有效、何时有效以及为什么有效知之甚少。本综述描述了医疗整合计划,这是朝着对医疗整合进行结构化研究迈出的第一步。