Department of Gastrointestinal Surgery, Peking University Shougang Hospital, No.9 Jinyuanzhuang Road, Shijingshan District, Beijing, China.
Center for Precision Diagnosis and Treatment of Colorectal Cancer and Inflammatory Disease, Peking University Health Science Center, Beijing, China.
J Transl Med. 2023 Jan 30;21(1):63. doi: 10.1186/s12967-023-03884-3.
Circulating tumor DNA (ctDNA) detection following curative-intent surgery could directly reflect the presence of minimal residual disease, the ultimate cause of clinical recurrence. However, ctDNA is not postoperatively detected in ≥ 50% of patients with stage I-III colorectal cancer (CRC) who ultimately recur. Herein we sought to improve recurrence risk prediction by combining ctDNA with clinicopathological risk factors in stage I-III CRC.
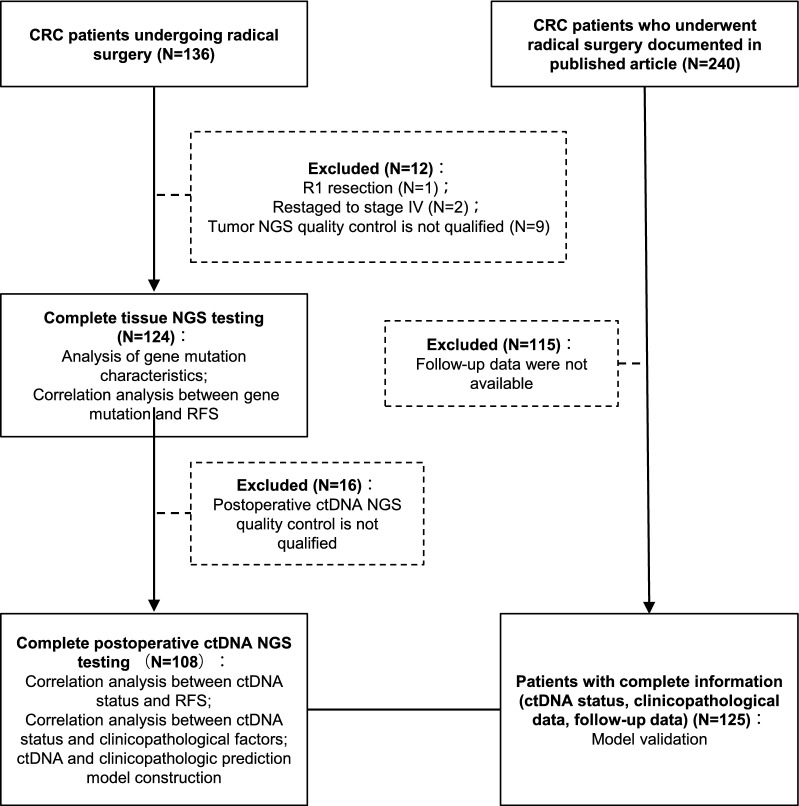
Two independent cohorts, both consisting of early-stage CRC patients who underwent curative surgery, were included: (i) the discovery cohort (N = 124) with tumor tissues and postoperative plasmas for ctDNA determination; and (ii) the external validation cohort (N = 125) with available ctDNA results. In the discovery cohort, somatic variations in tumor tissues and plasmas were determined via a 733-gene and 127-gene next-generation sequencing panel, respectively.
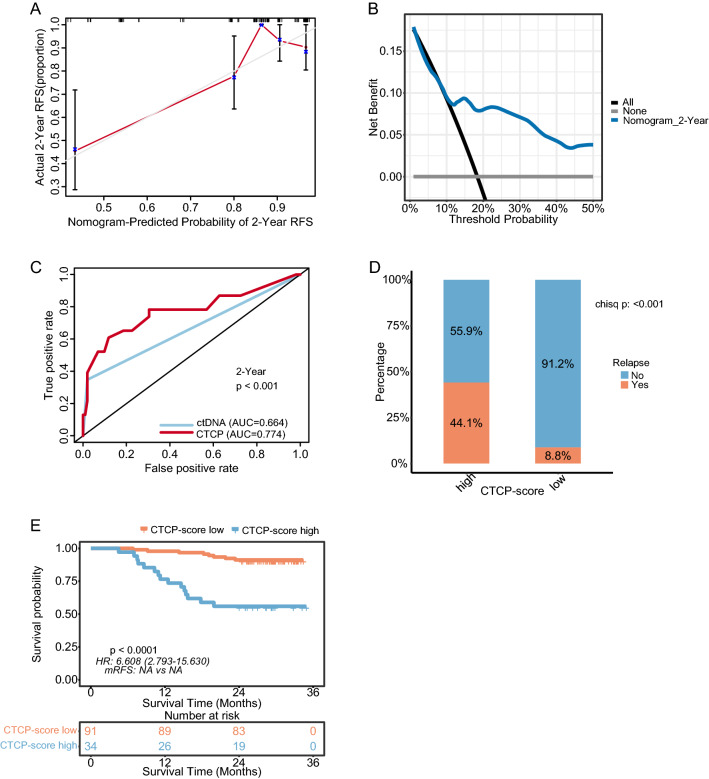
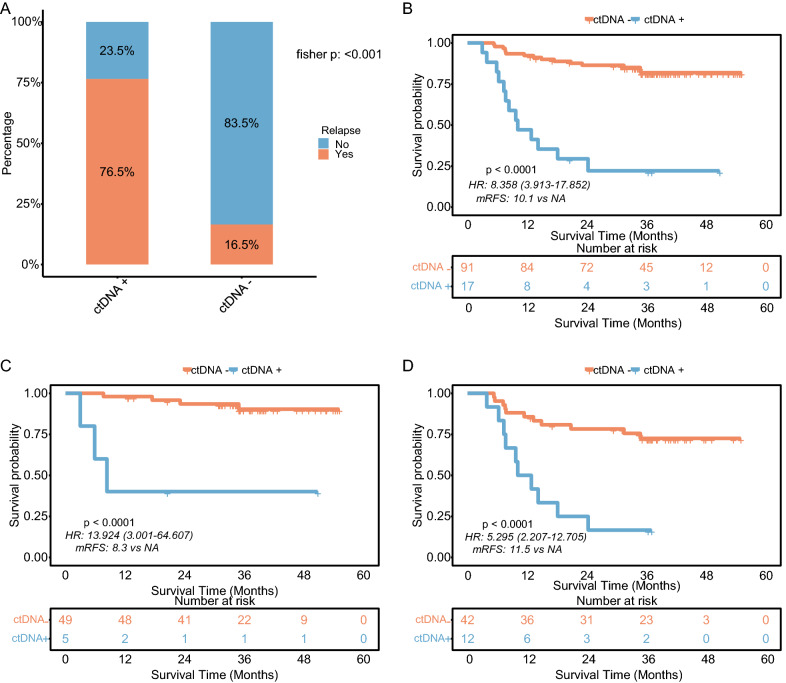
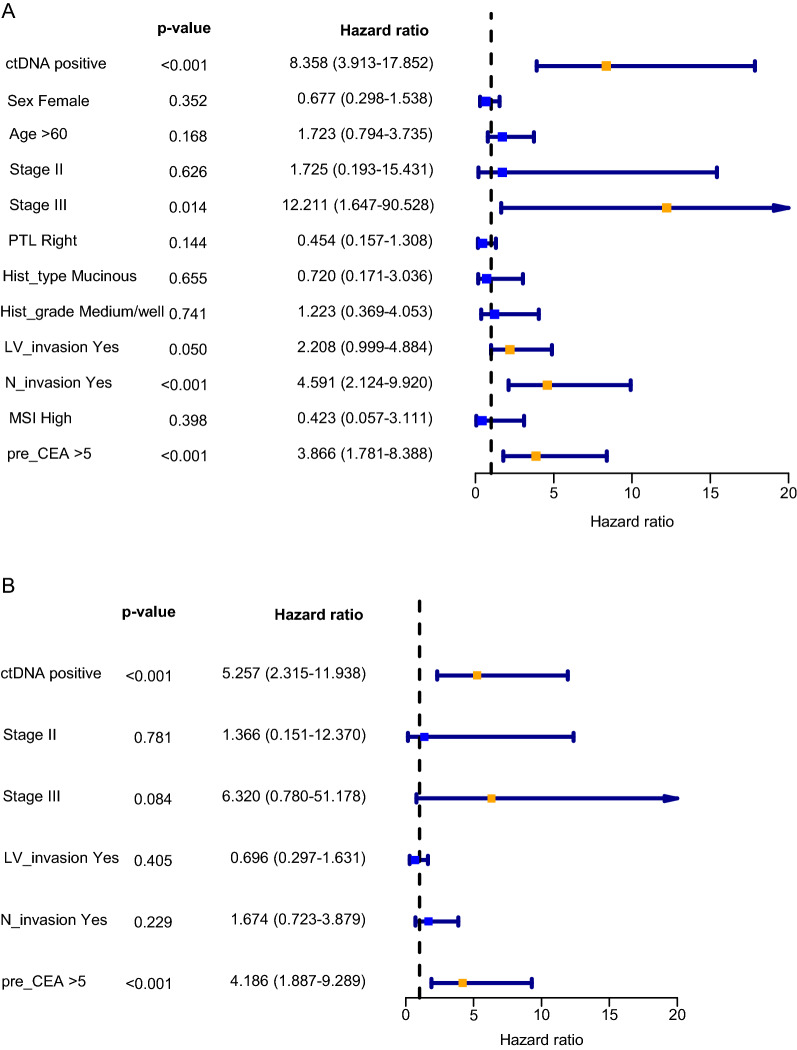
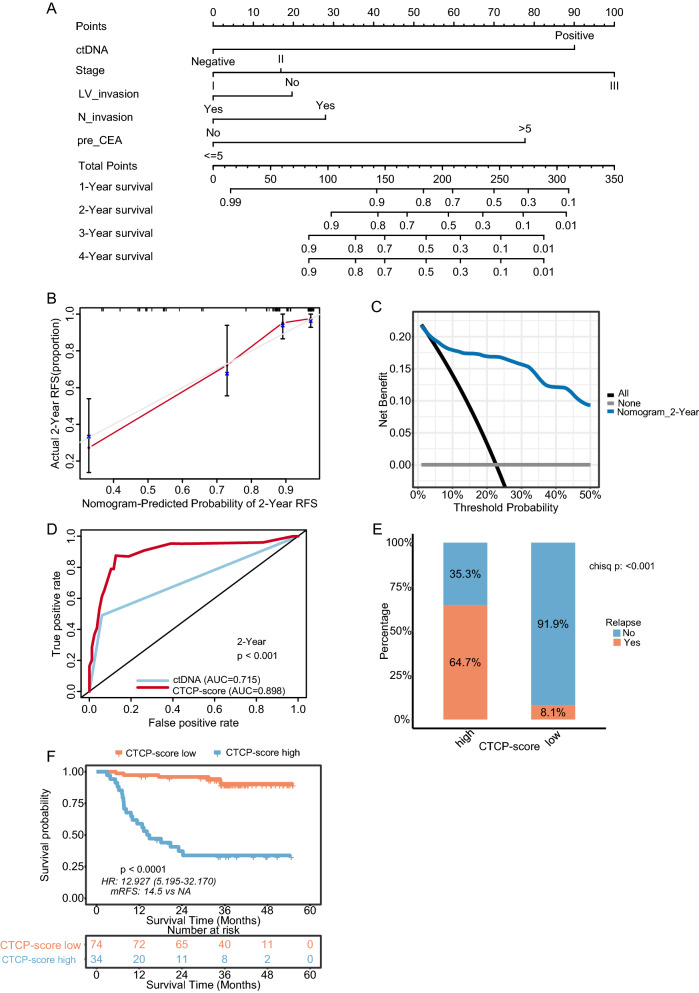
In the discovery cohort, 17 of 108 (15.7%) patients had detectable ctDNA. ctDNA-positive patients had a significantly high recurrence rate (76.5% vs. 16.5%, P < 0.001) and short recurrence-free survival (RFS; P < 0.001) versus ctDNA-negative patients. In addition to ctDNA status, the univariate Cox model identified pathologic stage, lymphovascular invasion, nerve invasion, and preoperative carcinoembryonic antigen level associated with RFS. We combined the ctDNA and clinicopathological risk factors (CTCP) to construct a model for recurrence prediction. A significantly higher recurrence rate (64.7% vs. 8.1%, P < 0.001) and worse RFS (P < 0.001) were seen in the high-risk patients classified by the CTCP model versus those in the low-risk patients. Receiver operating characteristic analysis demonstrated that the CTCP model outperformed ctDNA alone at recurrence prediction, which increased the sensitivity of 2 year RFS from 49.6% by ctDNA alone to 87.5%. Harrell's concordance index, calibration curve, and decision curve analysis also suggested that the CTCP model had good discrimination, consistency, and clinical utility. These results were reproduced in the validation cohort.
Combining postoperative ctDNA and clinical risk may better predict recurrence than ctDNA alone for developing a personalized postoperative management strategy for CRC.
根治性手术后循环肿瘤 DNA(ctDNA)的检测可直接反映微小残留疾病的存在,而微小残留疾病是临床复发的最终原因。然而,在最终复发的 I 期-III 期结直肠癌(CRC)患者中,ctDNA 在≥50%的患者中无法检测到。在此,我们试图通过将 ctDNA 与 I 期-III 期 CRC 的临床病理危险因素相结合来提高复发风险预测。
本研究纳入了两个独立的队列,均由接受根治性手术的早期 CRC 患者组成:(i)包含 124 名患者的发现队列,对其肿瘤组织和术后血浆进行 ctDNA 检测;(ii)包含 125 名患者的外部验证队列,提供了 ctDNA 检测结果。在发现队列中,通过 733 基因和 127 基因下一代测序面板分别检测肿瘤组织和血浆中的体细胞变异。
在发现队列中,108 名患者中有 17 名(15.7%)可检测到 ctDNA。ctDNA 阳性患者的复发率(76.5%比 16.5%,P<0.001)和无复发生存率(RFS;P<0.001)显著高于 ctDNA 阴性患者。除了 ctDNA 状态外,单因素 Cox 模型还确定了病理分期、脉管侵犯、神经侵犯和术前癌胚抗原水平与 RFS 相关。我们将 ctDNA 和临床病理危险因素(CTCP)相结合,构建了一种用于复发预测的模型。在根据 CTCP 模型分类的高风险患者中,复发率(64.7%比 8.1%,P<0.001)和 RFS 更差(P<0.001)。受试者工作特征分析表明,与 ctDNA 相比,CTCP 模型在预测复发方面表现更好,将 2 年 RFS 的敏感性从单独使用 ctDNA 的 49.6%提高到 87.5%。Harrell 一致性指数、校准曲线和决策曲线分析也表明,CTCP 模型具有良好的区分度、一致性和临床实用性。这些结果在验证队列中得到了重现。
与单独使用 ctDNA 相比,联合术后 ctDNA 和临床风险可以更好地预测 CRC 患者的复发,从而为制定个性化的术后管理策略提供依据。