Cancer Biology Research Center (Key Laboratory of the Ministry of Education), Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, China.
Department of Gynecology and Obstetrics, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, China.
Cancer Med. 2023 Apr;12(7):8897-8910. doi: 10.1002/cam4.5643. Epub 2023 Jan 31.
Stage IB (deep myometrial invasion) high-grade endometrioid adenocarcinoma (EA), regardless of LVSI status, is classified into high-intermediate risk groups, requiring surgical lymph node staging. Intraoperative frozen section (IFS) is commonly used, but its adequacy and reliability vary between reports. Hence, we determined the utility of IFS in identification of high-risk factors, including deep myometrial invasion and high-grade.
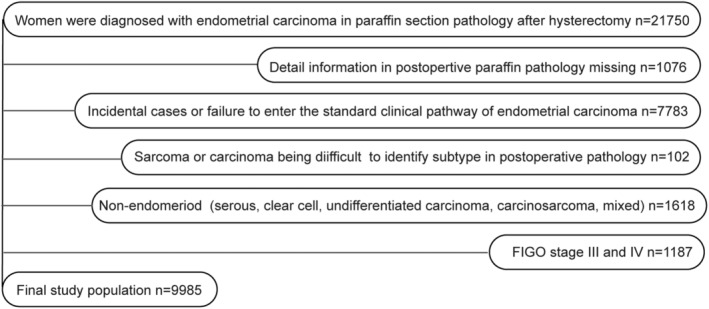
We retrospectively analyzed 9,985 cases operated with hysterectomy and diagnosed with FIGO stage I/II EA in postoperative paraffin section (PS) results at 30 Chinese hospitals from 2000 to 2019. We determined diagnostic performance of IFS and investigated whether the addition of IFS to preoperative biopsy and imaging could improve identification of high-risk factors.
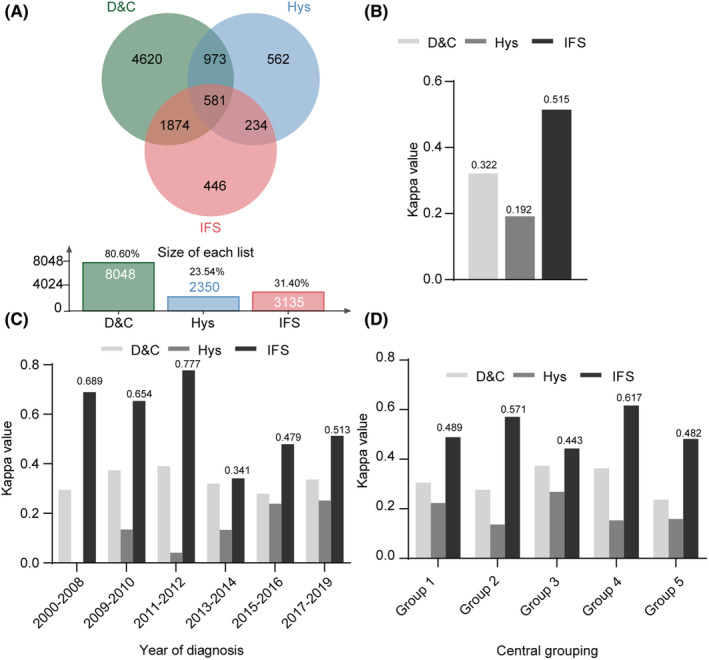
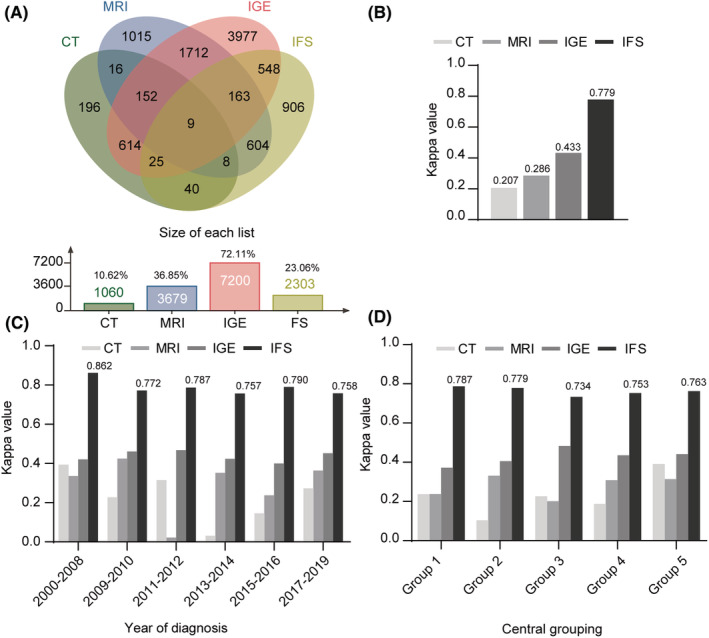
IFS and postoperative PS presented the highest concordance in assessing deep myometrial invasion (Kappa: 0.834), followed by intraoperative gross examination (IGE Kappa: 0.643), MRI (Kappa: 0.395), and CT (Kappa: 0.207). IFS and postoperative PS presented the highest concordance for high-grade EA (Kappa: 0.585) compared to diagnostic curettage (D&C 0.226) and hysteroscope (Hys 0.180). Sensitivity and specificity for detecting deep myometrial invasion were 86.21 and 97.20% for IFS versus 51.72 and 88.81% for MRI, 68.97 and 94.41% for IGE. These figures for detecting high-grade EA were 58.21 and 96.50% for IFS versus 16.42 and 98.83% for D&C, 13.43 and 98.64% for Hys. Parallel strategies, including MRI-IFS (Kappa: 0.626), D&C-IFS (Kappa: 0.595), and Hys-IFS (Kappa: 0.578) improved the diagnostic efficiencies of individual preoperative examinations. Based on the high sensitivity of IFS, parallel strategies improved the sensitivities of preoperative examinations to 89.66% (MRI), 64.18% (D&C), 62.69% (Hys), respectively, and these differences were statistically significant (p = 0.000).
IFS presented reasonable agreement rates predicting postoperative PS results, including deep myometrial invasion and high-grade. IFS helps identify high-intermediate risk patients in preoperative biopsy and MRI and guides intraoperative lymphadenectomy decisions in EA.
IB 期(深部肌层浸润)高级别子宫内膜腺癌(EA),无论 LVSI 状态如何,均被归类为高中危组,需要进行外科淋巴结分期。术中冰冻切片(IFS)常用于此,但在不同报道中的充分性和可靠性存在差异。因此,我们旨在确定 IFS 在识别高危因素(包括深部肌层浸润和高级别)方面的作用。
我们回顾性分析了 2000 年至 2019 年 30 家中国医院的 9985 例接受子宫切除术并在术后石蜡切片(PS)中诊断为 FIGO Ⅰ/Ⅱ期 EA 的患者。我们确定了 IFS 的诊断性能,并探讨了在术前活检和影像学中加入 IFS 是否可以提高高危因素的识别率。
IFS 和术后 PS 在评估深部肌层浸润方面具有最高的一致性(Kappa:0.834),其次是术中大体检查(IGE,Kappa:0.643)、MRI(Kappa:0.395)和 CT(Kappa:0.207)。IFS 和术后 PS 在评估高级别 EA 方面具有最高的一致性(Kappa:0.585),而与诊断性刮宫(D&C,Kappa:0.226)和宫腔镜(Hys,Kappa:0.180)相比。IFS 检测深部肌层浸润的灵敏度和特异度分别为 86.21%和 97.20%,而 MRI 为 51.72%和 88.81%,IGE 为 68.97%和 94.41%。IFS 检测高级别 EA 的灵敏度和特异度分别为 58.21%和 96.50%,而 D&C 为 16.42%和 98.83%,Hys 为 13.43%和 98.64%。MRI-IFS(Kappa:0.626)、D&C-IFS(Kappa:0.595)和 Hys-IFS(Kappa:0.578)等平行策略提高了单个术前检查的诊断效率。基于 IFS 的高灵敏度,这些平行策略将术前检查的灵敏度分别提高到 89.66%(MRI)、64.18%(D&C)和 62.69%(Hys),差异具有统计学意义(p=0.000)。
IFS 在预测术后 PS 结果(包括深部肌层浸润和高级别)方面具有合理的一致性。IFS 有助于在术前活检和 MRI 中识别中高危患者,并指导 EA 术中淋巴结切除术决策。