Department of Epidemiology, University of Washington, Seattle, Washington, USA.
Medical Research Council Centre for Global Infectious Disease Analysis, School of Public Health, Imperial College London.
AIDS. 2023 Apr 1;37(5):795-802. doi: 10.1097/QAD.0000000000003463. Epub 2023 Feb 3.
Voluntary medical male circumcision (VMMC) is an important component of combination HIV prevention. Inclusion of traditionally circumcised HIV negative men in VMMC uptake campaigns may be important if traditional male circumcision is less protective against HIV acquisition than VMMC.
We used data from the HIV Prevention Trials Network (HPTN) 071 (PopART) study. This cluster-randomized trial assessed the impact of a combination prevention package on population-level HIV incidence in 21 study communities in Zambia and South Africa. We evaluated uptake of VMMC, using a two-stage analysis approach and used discrete-time survival analysis to evaluate the association between the types of male circumcision and HIV incidence.
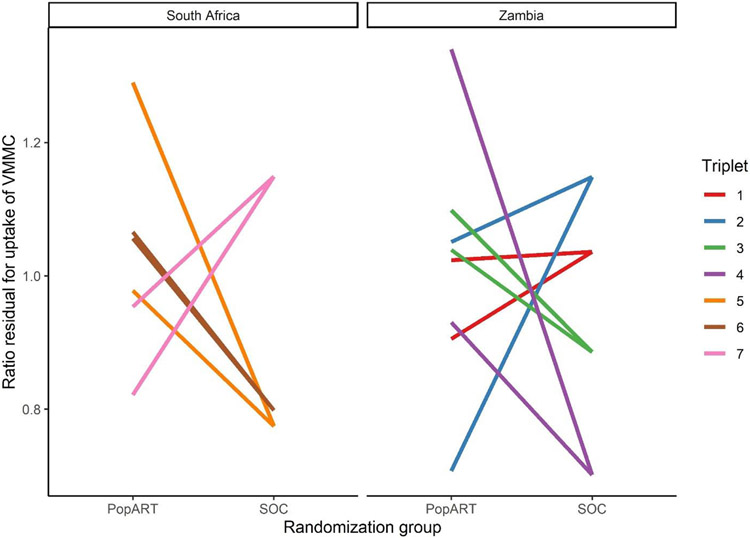
A total of 10 803 HIV-negative men with self-reported circumcision status were included in this study. At baseline, 56% reported being uncircumcised, 26% traditionally circumcised and 18% were medically circumcised. During the PopART intervention, 11% of uncircumcised men reported uptake of medical male circumcision. We found no significant difference in the uptake of VMMC in communities receiving the PopART intervention package and standard of care {adj. rate ratio=1·10 [95% confidence interval (CI) 0.82, 1.50, P = 0.48]}. The rate of HIV acquisition for medically circumcised men was 70% lower than for those who were uncircumcised adjusted hazard ratio (adjHR) = 0.30 (95% CI 0.16-0.55; P < 0.0001). There was no difference in rate of HIV acquisition for traditionally circumcised men compared to those uncircumcised adjHR = 0.84 (95% CI 0.54, 1.31; P = 0.45).
Household-based delivery of HIV testing followed by referral for medical male circumcision did not result in substantial VMMC uptake. Traditional circumcision is not associated with lower risk of HIV acquisition.
自愿男性包皮环切术(VMMC)是艾滋病综合防治的重要组成部分。如果传统男性包皮环切术对艾滋病病毒(HIV)的保护作用不如 VMMC,那么将传统上已行包皮环切术的 HIV 阴性男性纳入 VMMC 推广活动中可能非常重要。
我们使用了 HIV 预防试验网络(HPTN)071(PopART)研究的数据。这项集群随机试验评估了在赞比亚和南非的 21 个研究社区中,综合预防方案对人群 HIV 发病率的影响。我们使用两阶段分析方法评估 VMMC 的采用情况,并使用离散时间生存分析评估两种男性包皮环切术类型与 HIV 发病率之间的关联。
本研究共纳入了 10803 名自我报告有包皮环切史的 HIV 阴性男性。基线时,56%的人报告未行包皮环切术,26%的人报告行过传统包皮环切术,18%的人报告行过医学包皮环切术。在 PopART 干预期间,11%的未行包皮环切术的男性报告接受了医学男性包皮环切术。我们发现,接受 PopART 干预方案和标准护理的社区之间,VMMC 的采用率没有显著差异[调整后比值比(adjRR)=1.10(95%置信区间(CI)0.82,1.50,P=0.48)]。与未行包皮环切术的男性相比,行医学包皮环切术的男性 HIV 感染率降低了 70%(调整后危险比(adjHR)=0.30(95%CI 0.16-0.55;P <0.0001))。与未行包皮环切术的男性相比,行传统包皮环切术的男性 HIV 感染率没有差异(adjHR=0.84(95%CI 0.54,1.31;P=0.45))。
以家庭为基础的 HIV 检测后,再进行医学包皮环切术的推广并没有导致大量的 VMMC 采用。传统的包皮环切术与较低的 HIV 感染风险无关。