National Health Service Blood and Transplant, Bristol, United Kingdom.
UK Health Security Agency, London, United Kingdom.
Transplantation. 2023 May 1;107(5):1124-1135. doi: 10.1097/TP.0000000000004535. Epub 2023 Jan 25.
The effectiveness of vaccines against the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) B.1.1.529 Omicron variant in immunosuppressed solid organ and islet transplant (SOT) recipients is unclear.
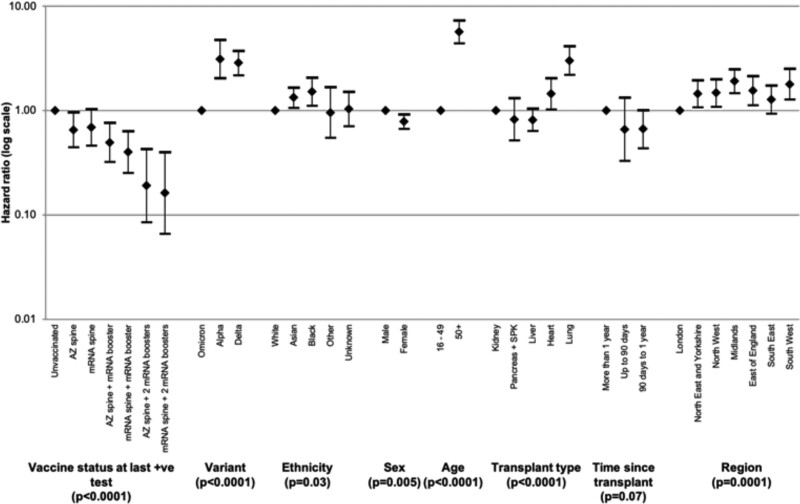
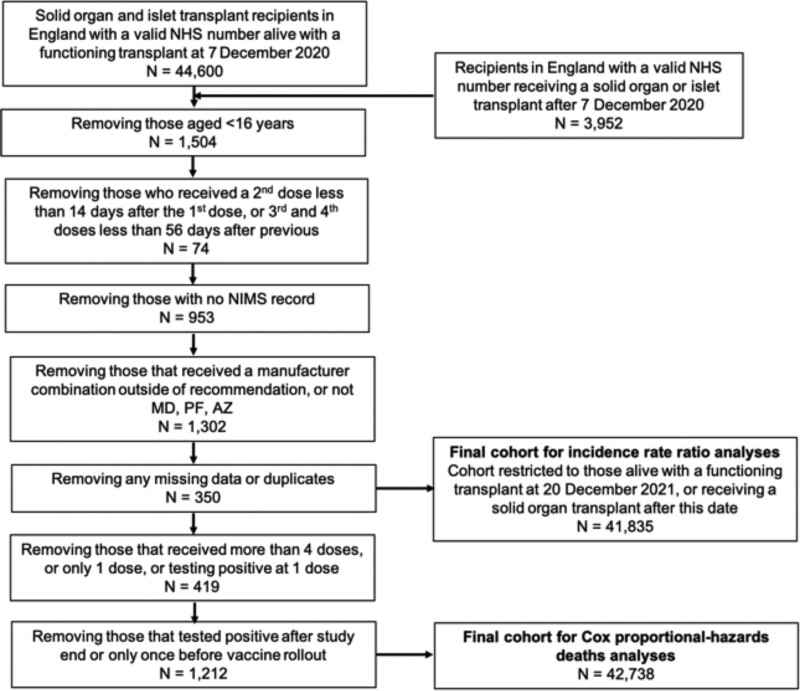
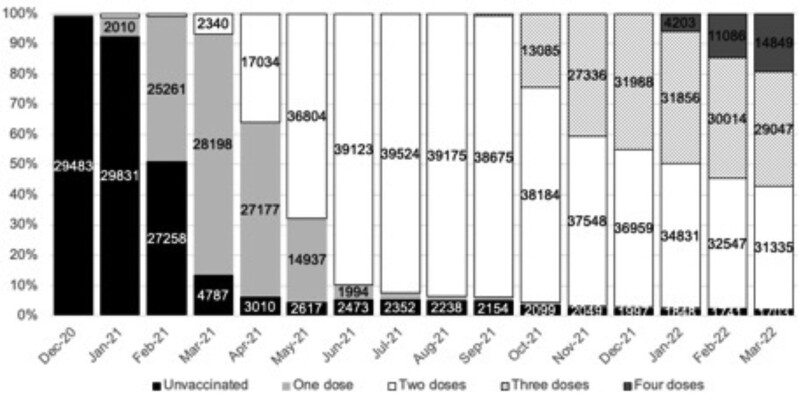
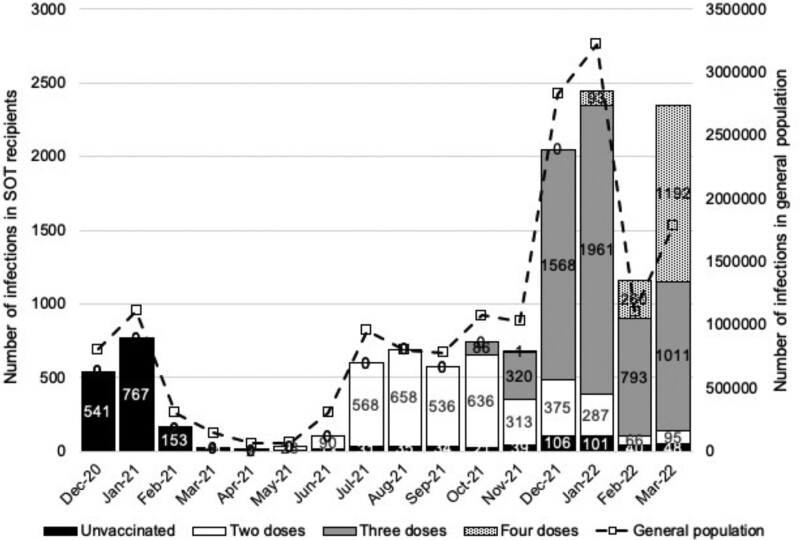
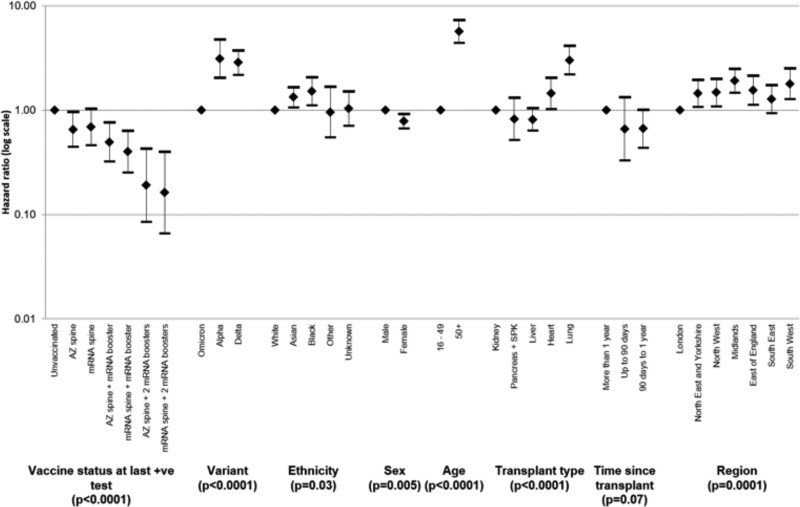
National registries in England were linked to identify SARS-CoV-2 positive tests, noninjury hospitalization within 14 d, and deaths within 28 d between December 7, 2020, and March 31, 2022 in adult SOT recipients. Incidence rate ratios (IRRs) for infection, and hospitalization or death, were adjusted for recipient demographics and calendar month for the Omicron-dominant period (December 20, 2021, to March 31, 2022). Mortality risk following SARS-CoV-2 infection was adjusted for recipient demographics and dominant variant using a Cox proportional-hazards model for the entire time period.
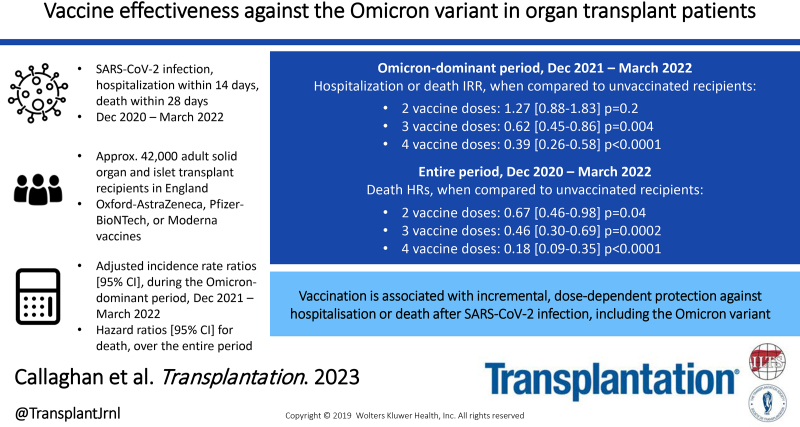
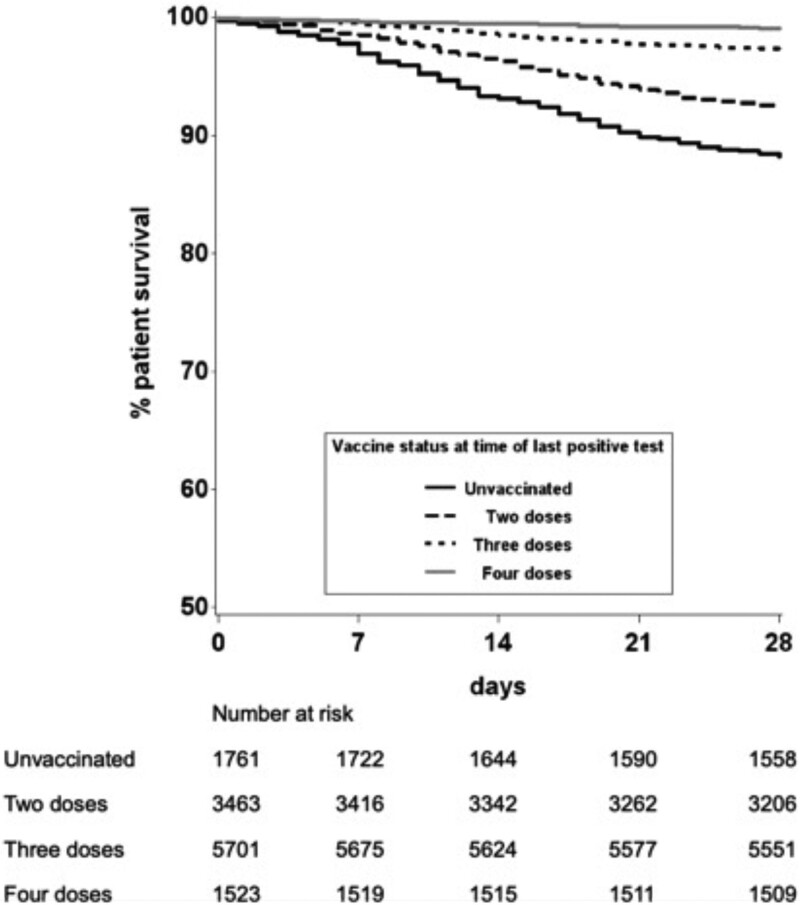
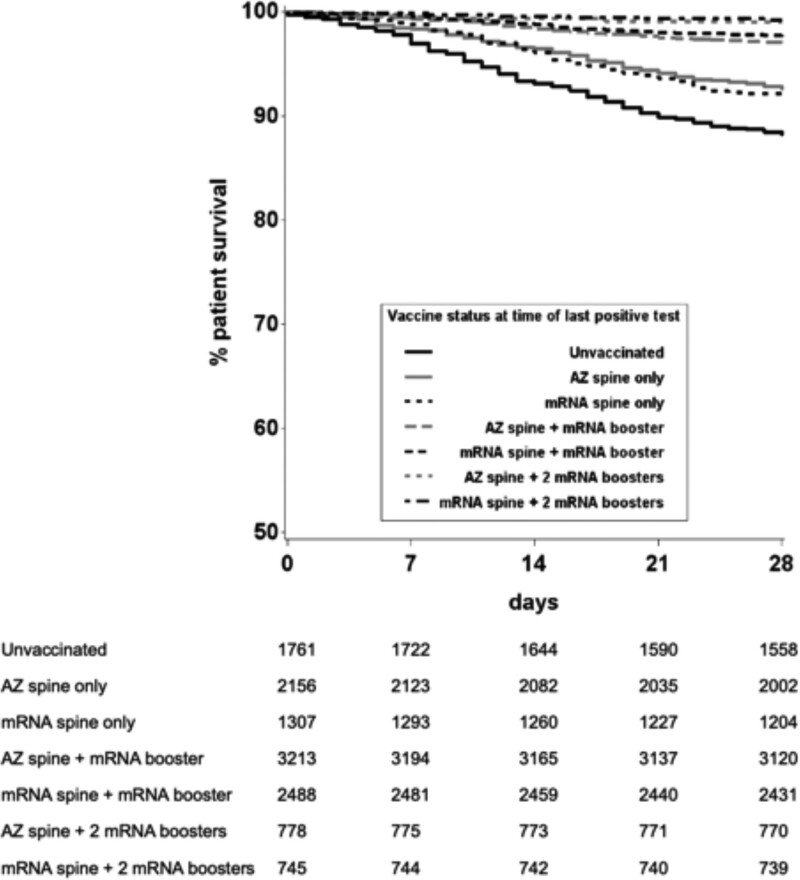
During the Omicron-dominant period, infection IRRs (95% confidence intervals) were higher in those receiving 2, 3, and 4 vaccine doses than in unvaccinated patients (1.25 [1.08-1.45], 1.46 [1.28-1.67], and 1.79 [1.54-2.06], respectively). However, hospitalization or death IRRs during this period were lower in those receiving 3 or 4 vaccine doses than in unvaccinated patients (0.62 [0.45-0.86] and 0.39 [0.26-0.58], respectively). Risk-adjusted analyses for deaths after SARS-CoV-2 infection between December 7, 2020, and March 31, 2022, found hazard ratios (95% confidence intervals) of 0.67 (0.46-0.98), 0.46 (0.30-0.69), and 0.18 (0.09-0.35) for those with 2, 3, and 4 vaccine doses, respectively, when compared with the unvaccinated group.
In immunosuppressed SOT recipients, vaccination is associated with incremental, dose-dependent protection against hospitalization or death after SARS-CoV-2 infection, including against the Omicron variant.
针对严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)B.1.1.529 奥密克戎变异株,免疫抑制的实体器官和胰岛移植(SOT)受者疫苗的有效性尚不清楚。
在 2020 年 12 月 7 日至 2022 年 3 月 31 日期间,通过英格兰国家登记处将 SARS-CoV-2 阳性检测、14 天内非创伤性住院和 28 天内死亡与成人 SOT 受者联系起来。在奥密克戎主导期间,调整了感染率(IRR)和住院或死亡的 IRR,调整因素包括受者人口统计学和日历月份。使用 Cox 比例风险模型,对整个时期的 SARS-CoV-2 感染后死亡率进行了受者人口统计学和优势变异的调整。
在奥密克戎主导期间,与未接种疫苗的患者相比,接受 2、3 和 4 剂疫苗的患者感染 IRR(95%置信区间)更高(分别为 1.25[1.08-1.45]、1.46[1.28-1.67]和 1.79[1.54-2.06])。然而,在此期间,接受 3 或 4 剂疫苗的患者住院或死亡的 IRR 低于未接种疫苗的患者(分别为 0.62[0.45-0.86]和 0.39[0.26-0.58])。对 2020 年 12 月 7 日至 2022 年 3 月 31 日期间 SARS-CoV-2 感染后死亡的风险调整分析发现,与未接种疫苗组相比,接受 2、3 和 4 剂疫苗的患者的风险比(95%置信区间)分别为 0.67(0.46-0.98)、0.46(0.30-0.69)和 0.18(0.09-0.35)。
在免疫抑制的 SOT 受者中,疫苗接种与 SARS-CoV-2 感染后住院或死亡的剂量依赖性保护作用相关,包括对奥密克戎变异株的保护作用。