Leeds Institute for Cardiovascular and Metabolic Medicine, University of Leeds, Leeds, UK.
Leeds Institute of Data Analytics, University of Leeds, Leeds, UK.
ESC Heart Fail. 2023 Apr;10(2):1372-1384. doi: 10.1002/ehf2.14290. Epub 2023 Feb 3.
Prognosis for ST-segment elevation myocardial infarction (STEMI) is worse when heart failure is present on admission. Understanding clinical practice in different health systems can identify areas for quality improvement initiatives to improve outcomes. In the absence of international comparison studies, we aimed to compare treatments and in-hospital outcomes of patients admitted with ST elevation myocardial infarction (STEMI) by heart failure status in two healthcare-wide cohorts.
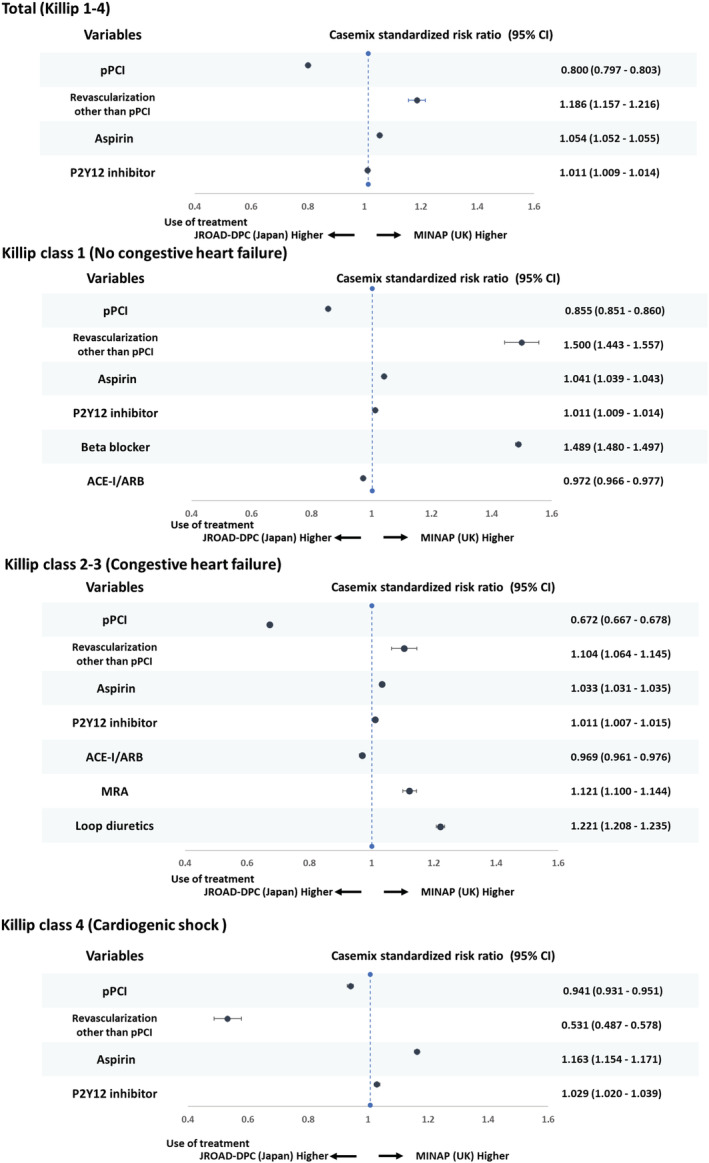
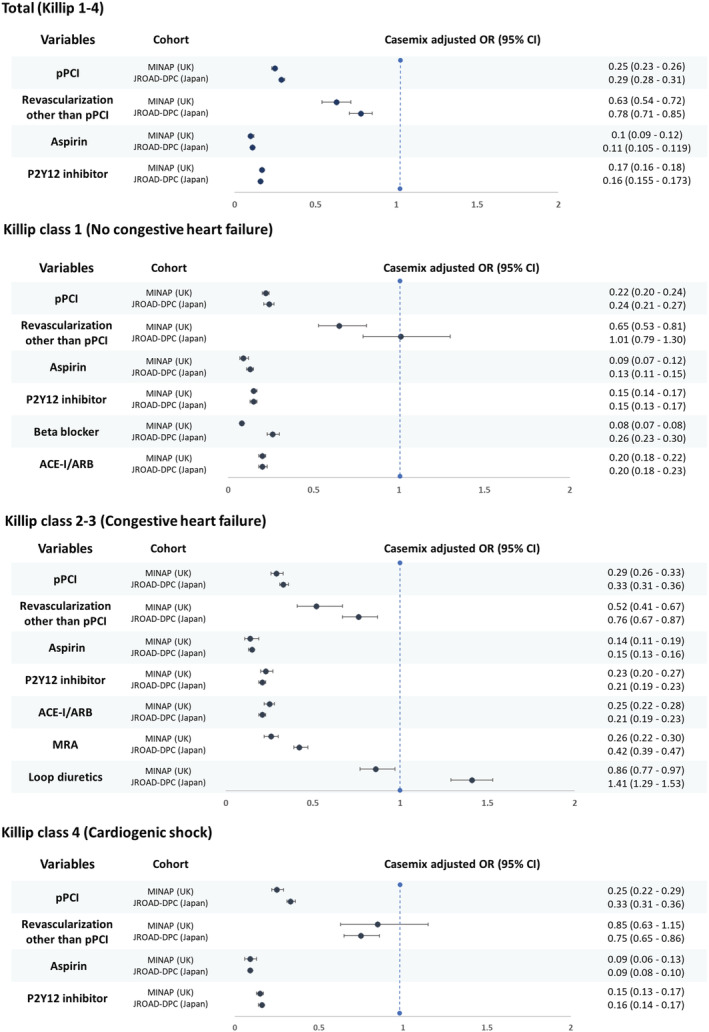
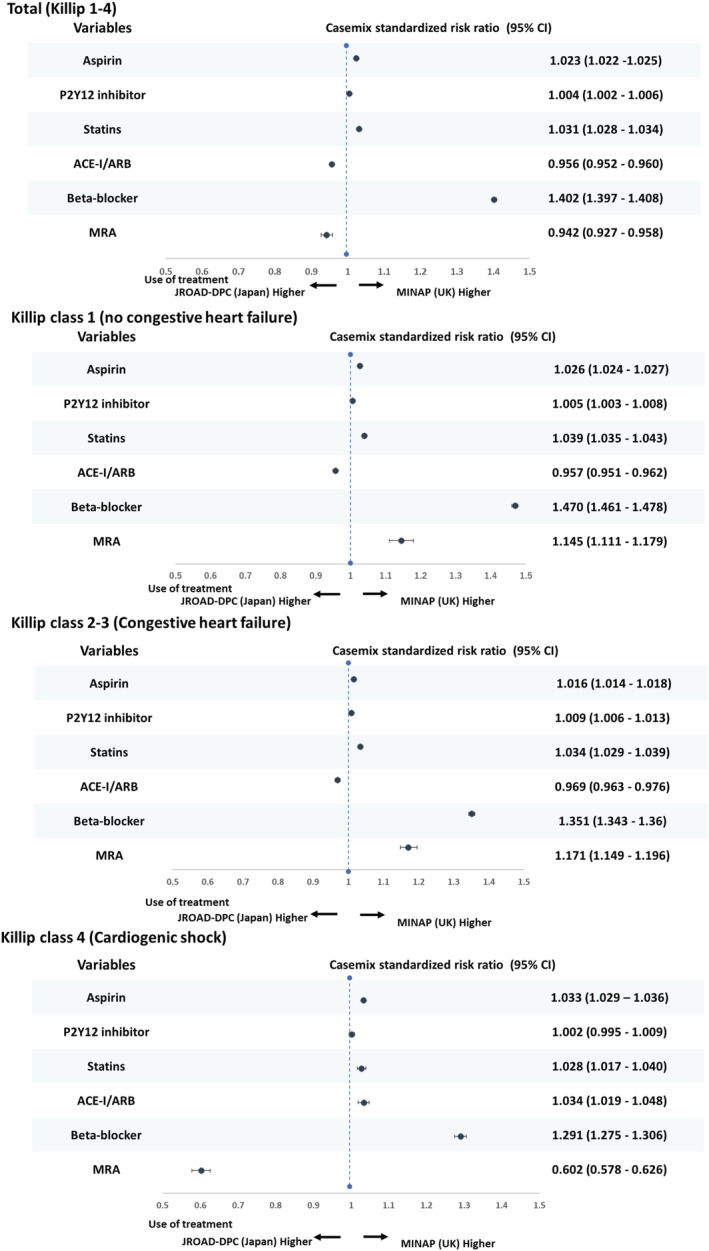
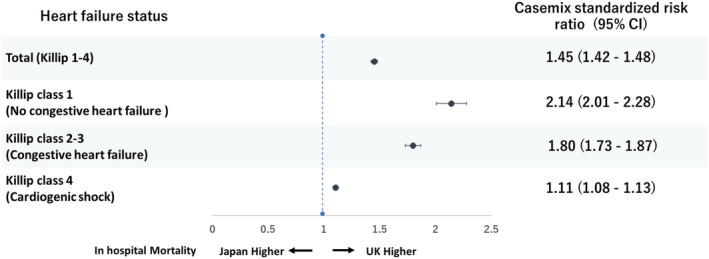
We used two nationwide databases to capture admissions with STEMI in the United Kingdom (Myocardial ischemia National Audit Project, MINAP) and Japan (Japanese Registry of All Cardiac and Vascular Diseases-Diagnostic Procedure Combination, JROAD-DPC) between 2012 and 2017. Participants were stratified using the HF Killip classification into three groups; Killip 1: no congestive heart failure, Killip 2-3: congestive heart failure, Killip 4: cardiogenic shock. We calculated crude rate and case mix standardized risk ratios (CSRR) for use of treatments and in-hospital death. Patients were younger in the United Kingdom (65.4 [13.6] vs. 69.1 [13.0] years) and more likely to have co-morbidities in the United Kingdom except for diabetes and hypertension. Japan had a higher percentage of heart failure and cardiogenic shock patients among STEMI during admission than that in the United Kingdom. Primary percutaneous coronary intervention (pPCI) rates were lower in the United Kingdom compared with Japan, especially for patients presenting with Killip 2-3 class heart failure (pPCI use in patients with Killip 1, 2-3, 4: Japan, 86.2%, 81.7%, 78.7%; United Kingdom, 79.6%, 58.2% and 79.9%). In contrast, beta-blocker use was consistently lower in Japan than in the United Kingdom (61.4% vs. 90.2%) across Killip classifications and length of hospital stay longer (17.0 [9.7] vs. 5.0 [7.4] days). The crude rate of in-hospital mortality increased with increasing Killip class group. Both the crude rate and CSRR was higher in the United Kingdom compared with Japan for Killip 2-3 (15.8% vs. 6.4%, CSRR 1.80 95% CI 1.73-1.87, P < 0.001), and similar for Killip 4 (36.9% vs. 36.3%, CSRR 1.11 95% CI 1.08-1.13, P < 0.001).
Important differences in the care and outcomes for STEMI with heart failure exist between the United Kingdom and Japan. Specifically, in the United Kingdom, there was a lower rate of pPCI, and in Japan, fewer patients were prescribed beta blockers and hospital length of stay was longer. This international comparison can inform targeted quality improvement programmes to narrow the outcome gap between health systems.
当入院时存在心力衰竭时,ST 段抬高型心肌梗死(STEMI)的预后更差。了解不同医疗体系中的临床实践情况,可以确定质量改进举措的领域,以改善结果。由于缺乏国际比较研究,我们旨在通过两个全医疗范围的队列,比较心力衰竭状态下因 ST 段抬高型心肌梗死(STEMI)入院的患者的治疗和院内结局。
我们使用两个全国性数据库(英国心肌缺血国家审计项目(MINAP)和日本所有心血管疾病注册-诊断程序组合(JROAD-DPC)),在 2012 年至 2017 年间捕获 STEMI 入院患者。参与者使用心力衰竭 Killip 分级分为三组;Killip 1:无充血性心力衰竭,Killip 2-3:充血性心力衰竭,Killip 4:心源性休克。我们计算了治疗和院内死亡的粗率和病例混合标准化风险比(CSRR)。与英国相比,日本患者入院时更年轻(65.4 [13.6] 岁 vs. 69.1 [13.0] 岁),且除糖尿病和高血压外,更可能伴有合并症。与英国相比,日本因 STEMI 入院的心力衰竭和心源性休克患者比例更高。与日本相比,英国的经皮冠状动脉介入治疗(pPCI)率较低,尤其是对于 Killip 2-3 级心力衰竭的患者(Killip 1、2-3、4 级患者的 pPCI 使用率:日本为 86.2%、81.7%、78.7%;英国为 79.6%、58.2%和 79.9%)。相反,β受体阻滞剂的使用在日本始终低于英国(Killip 分级和住院时间的 61.4% vs. 90.2%)(61.4% vs. 90.2%)。与英国相比,日本的住院死亡率随着 Killip 级别的增加而增加。与日本相比,英国的 Killip 2-3 级的死亡率均较高(15.8% vs. 6.4%,CSRR 1.80,95%CI 1.73-1.87,P<0.001),Killip 4 级的死亡率相似(36.9% vs. 36.3%,CSRR 1.11,95%CI 1.08-1.13,P<0.001)。
英国和日本在心力衰竭 STEMI 的治疗和结局方面存在重要差异。具体来说,在英国,pPCI 率较低,而在日本,β受体阻滞剂的使用率较低,住院时间较长。这种国际比较可以为质量改进计划提供信息,以缩小不同医疗体系之间的结果差距。