Du Lin, Ernani Vinicius, Liu Alex, Schild Steven E, Jaroszewski Dawn E, Cassivi Steven D, Beamer Staci E, Luo Yung-Hung, Wampfler Jason A, Santos Pedro A Reck Dos, Wigle Dennis, Sun Daqiang, Shen K Robert, Yang Ping
Department of Thoracic Surgery, Tianjin Chest Hospital, Tianjin 300222, P.R. China.
Division of Epidemiology, Department of Quantitative Health Sciences, Mayo Clinic, Scottsdale, AZ 85260, USA.
Oncol Lett. 2023 Jan 10;25(2):80. doi: 10.3892/ol.2023.13666. eCollection 2023 Feb.
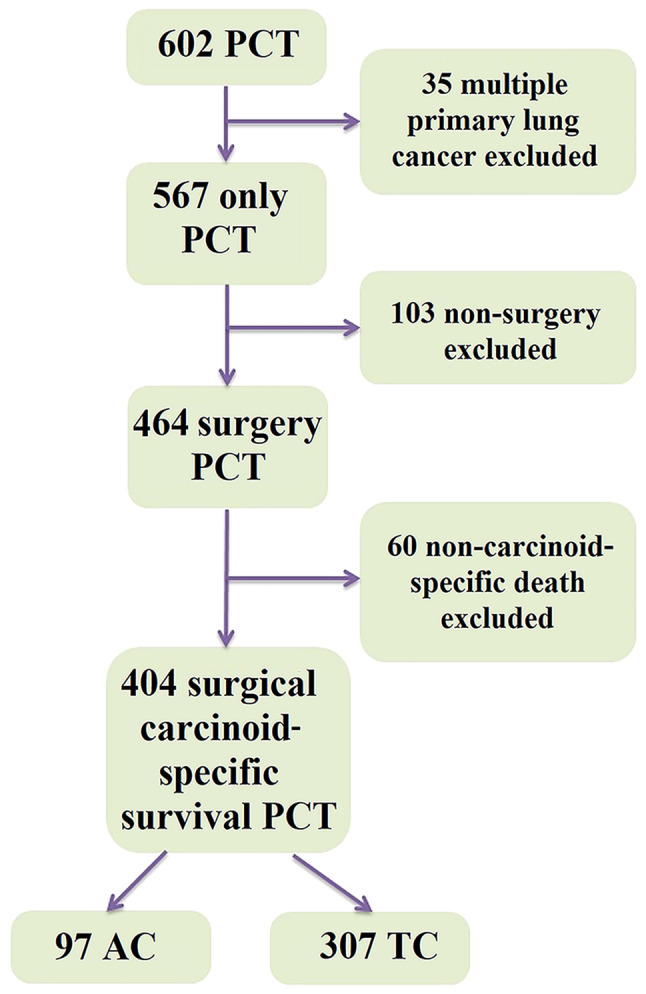
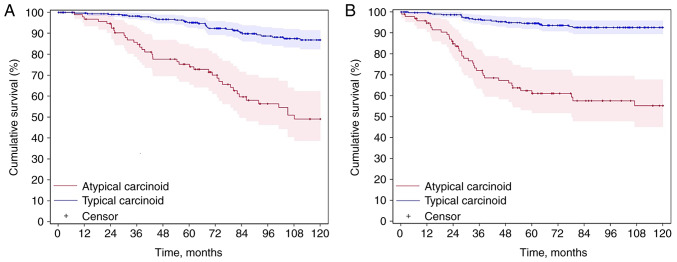
The objective of the present study was to characterize the difference in 10-year carcinoid-specific survival (CSS) and disease-free survival (DFS) among patients with resected pulmonary typical carcinoid (TC) and atypical carcinoid (AC). Patients diagnosed with pulmonary carcinoid tumors (PCT) between January 1, 1997, and December 31, 2016, were identified. All patients underwent video-assisted thoracoscopic surgery or thoracotomy with thoracic lymphadenectomy. Cumulative CSS was estimated using the Kaplan-Meier model. The analysis of hazard ratios (HRs) and 95% confidence intervals (CIs) was performed using univariate and multivariate Cox proportional hazards models. A total of 404 patients with PCT were included in the present study. The 10-year CSS and DFS rates of patients with AC were significantly worse than those of patients with TC (49.1 vs. 86.8% and 52.2 vs. 92.6%, respectively; P<0.001). In the CSS multivariate analysis, older age and lymph node involvement (HR, 2.45; P=0.022) were associated with worse survival in AC, while age, male sex, M1 stage, cigarette smoking and inadequate N2 lymphadenectomy were associate with worse survival in TC. In the recurrence multivariate analysis, N1-3 stage (HR, 2.62; 95% CI, 1.16-5.95; P=0.018) and inadequate N2 lymphadenectomy (HR, 2.13; 95% CI, 1.04-4.39; P=0.041) were associated with an increase in recurrence in AC, while male sex (HR, 3.72; 95% CI, 1.33-10.42; P=0.010) and M1 stage (HR, 14.93; 95% CI, 4.77-46.77; P<0.001) were associated with an increase in recurrence in TC. In conclusion, patients with AC tumors had significantly worse CSS and DFS rates compared with patients with TC. The degree of nodal involvement in AC was a prognostic marker, in contrast to that in TC. Inadequate lymphadenectomy increased the risk of recurrence in AC and mortality in TC, although surgical approaches did not have a significant impact. The present study therefore emphasizes the importance of mediastinal nodal dissection in patients with PCTs.
本研究的目的是描述接受手术切除的肺典型类癌(TC)和非典型类癌(AC)患者10年类癌特异性生存率(CSS)和无病生存率(DFS)的差异。确定了1997年1月1日至2016年12月31日期间诊断为肺类癌肿瘤(PCT)的患者。所有患者均接受了电视辅助胸腔镜手术或开胸手术及胸段淋巴结清扫术。使用Kaplan-Meier模型估计累积CSS。使用单因素和多因素Cox比例风险模型进行风险比(HRs)和95%置信区间(CIs)分析。本研究共纳入404例PCT患者。AC患者的10年CSS和DFS率显著低于TC患者(分别为49.1%对86.8%和52.2%对92.6%;P<0.001)。在CSS多因素分析中,年龄较大和淋巴结受累(HR,2.45;P=0.022)与AC患者较差的生存率相关,而年龄、男性、M1期、吸烟和N2淋巴结清扫不充分与TC患者较差的生存率相关。在复发多因素分析中,N1-3期(HR,2.62;95%CI,1.16-5.95;P=0.018)和N2淋巴结清扫不充分(HR,2.13;95%CI,1.04-4.39;P=0.041)与AC患者复发增加相关,而男性(HR,3.72;95%CI,1.33-10.42;P=0.010)和M1期(HR,14.93;95%CI,4.77-46.77;P<0.001)与TC患者复发增加相关。总之,与TC患者相比,AC肿瘤患者的CSS和DFS率显著更差。与TC不同,AC中淋巴结受累程度是一个预后标志物。淋巴结清扫不充分增加了AC患者复发风险和TC患者死亡风险,尽管手术方式没有显著影响。因此,本研究强调了纵隔淋巴结清扫在PCT患者中的重要性。