Louis Gilles, Schleich Florence, Guillaume Michèle, Kirkove Delphine, Nekoee Zahrei Halehsadat, Donneau Anne-Françoise, Henket Monique, Paulus Virginie, Guissard Françoise, Louis Renaud, Pétré Benoit
Department of Public Health, University of Liège, Liege, Belgium.
Department of Pneumology, GIGAI3, University of Liège, Liege, Belgium.
ERJ Open Res. 2023 Feb 6;9(1). doi: 10.1183/23120541.00451-2022. eCollection 2023 Jan.
Although asthma is a common disease, its diagnosis remains a challenge in clinical practice with both over- and underdiagnosis. Here, we performed a prospective observational study investigating the value of symptom intensity scales alone or combined with spirometry and exhaled nitric oxide fraction ( ) to aid in asthma diagnosis.
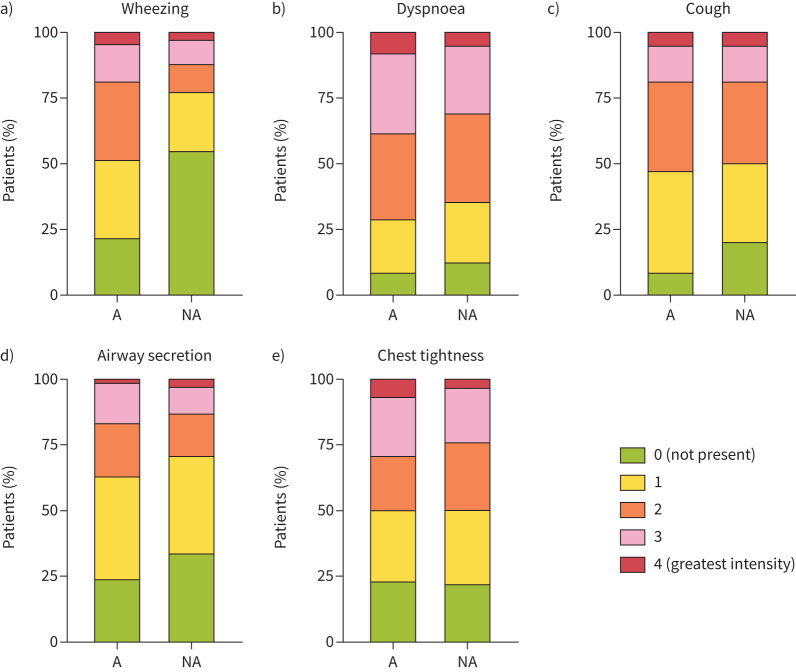
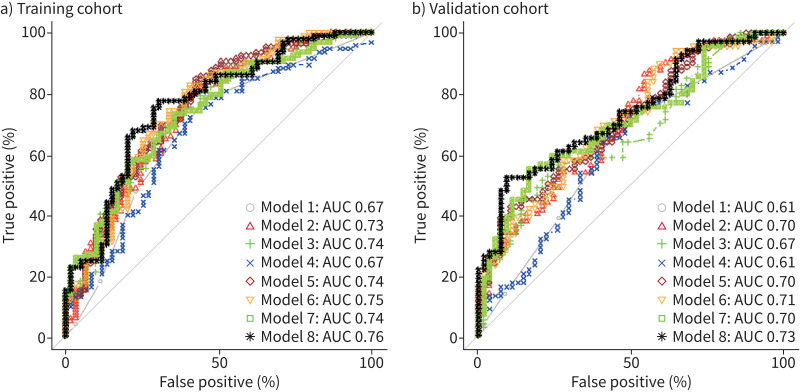
Over a 38-month period we recruited 303 untreated patients complaining of symptoms suggestive of asthma (wheezing, dyspnoea, cough, sputum production and chest tightness). The whole cohort was split into a training cohort (n=166) for patients recruited during odd months and a validation cohort (n=137) for patients recruited during even months. Asthma was diagnosed either by a positive reversibility test (≥12% and ≥200 mL in forced expiratory volume in 1 s (FEV)) and/or a positive bronchial challenge test (provocative concentration of methacholine causing a 20% fall in FEV ≤8 mg·mL). In order to assess the diagnostic performance of symptoms, spirometric indices and , we performed receiver operating characteristic curve analysis and multivariable logistic regression to identify the independent factors associated with asthma in the training cohort. Then, the derived predictive models were applied to the validation cohort.
63% of patients in the derivation cohort and 58% of patients in the validation cohort were diagnosed as being asthmatic. After logistic regression, wheezing was the only symptom to be significantly associated with asthma. Similarly, FEV (% pred), FEV/forced vital capacity (%) and were significantly associated with asthma. A predictive model combining these four parameters yielded an area under the curve of 0.76 (95% CI 0.66-0.84) in the training cohort and 0.73 (95% CI 0.65-0.82) when applied to the validation cohort.
Combining a wheezing intensity scale with spirometry and may help in improving asthma diagnosis accuracy in clinical practice.
尽管哮喘是一种常见疾病,但在临床实践中,其诊断仍然是一项挑战,存在过度诊断和诊断不足的情况。在此,我们进行了一项前瞻性观察性研究,调查单独使用症状强度量表或结合肺功能测定和呼出一氧化氮分数( )辅助哮喘诊断的价值。
在38个月的时间里,我们招募了303名未经治疗的患者,他们主诉有提示哮喘的症状(喘息、呼吸困难、咳嗽、咳痰和胸闷)。整个队列被分为一个训练队列(n = 166),用于奇数月招募的患者,以及一个验证队列(n = 137),用于偶数月招募的患者。哮喘通过阳性可逆性试验(一秒用力呼气量(FEV)增加≥12%且≥200 mL)和/或阳性支气管激发试验(引起FEV下降20%的乙酰甲胆碱激发浓度≤8 mg·mL)进行诊断。为了评估症状、肺功能指标和 的诊断性能,我们进行了受试者操作特征曲线分析和多变量逻辑回归,以确定训练队列中与哮喘相关的独立因素。然后,将推导的预测模型应用于验证队列。
推导队列中63%的患者和验证队列中58%的患者被诊断为哮喘。经过逻辑回归分析,喘息是唯一与哮喘显著相关的症状。同样,FEV(%预计值)、FEV/用力肺活量(%)和 与哮喘显著相关。结合这四个参数的预测模型在训练队列中的曲线下面积为0.76(95%可信区间0.66 - 0.84),应用于验证队列时为0.73(95%可信区间0.65 - 0.82)。
将喘息强度量表与肺功能测定和 相结合可能有助于提高临床实践中哮喘诊断的准确性。