Soriano Alex, Montravers Philippe, Bassetti Matteo, Klyasova Galina, Daikos George, Irani Paurus, Stone Gregory, Chambers Richard, Peeters Pascale, Shah Mitesh, Hulin Claire, Albuquerque Natalia, Basin Efim, Gaborit Benjamin, Kourbeti Irene, Menichetti Francesco, Perez-Rodriguez María Teresa, Pletz Mathias W, Sanchez Marisa, Trompa Ivan, Verma Anita, de Figueiredo Maria Lavinea N, Charbonneau Claudie
Department of Infectious Diseases, Hospital Clínic, Helios Building, Villarroel 170, Barcelona, Spain.
Department of Anaesthesiology and Surgical Critical Care Unit, CHU Bichat Claude Bernard, Assistance Publique-Hôpitaux de Paris, Université de Paris-Cité, Paris, France.
Infect Dis Ther. 2023 Mar;12(3):891-917. doi: 10.1007/s40121-023-00762-9. Epub 2023 Feb 10.
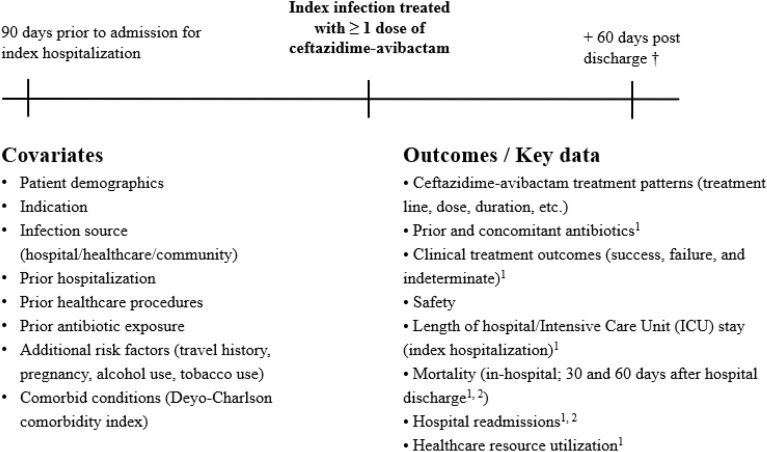
Ceftazidime-avibactam has proven activity against multidrug-resistant (MDR) bacteria in clinical trials and real-world studies. This study was conducted to describe the patterns of use of ceftazidime-avibactam (including indications and associated antibiotics), and the effectiveness and safety of ceftazidime-avibactam in real-world clinical practice.
This non-interventional medical chart review study was conducted in 11 countries across the European and Latin American (LATAM) regions. Consecutive patients treated in clinical practice with at least one dose of ceftazidime-avibactam for an approved indication per country label since 01 January 2018 (or launch date in the country if posterior) were enrolled. Effectiveness analyses were conducted in patients treated with ceftazidime-avibactam for at least 72 h.
Of the 569 eligible patients enrolled, 516 (90.7%) were treated for at least 72 h (354 patients from Europe and 162 patients from LATAM); 390 patients (75.7%) had switched from another antibiotic line for Gram-negative coverage. Infection sources were intra-abdominal, urinary, respiratory, bloodstream infections, and other infections (approximately 20% each). K. pneumoniae was the most common microorganism identified in the latest microbiological evaluation before starting ceftazidime-avibactam (59.3%). Two-thirds of microorganisms tested for susceptibility were MDR, of which 89.3% were carbapenem-resistant. The common MDR mechanisms for K. pneumoniae were carbapenemase (33.9%), oxacillinase 48 (25.2%), extended-spectrum beta-lactamase (21.5%), or metallo-beta-lactamase (14.2%) production. Without prior patient exposure, 17 isolates (mostly K. pneumoniae) were resistant to ceftazidime-avibactam. Treatment success was achieved in 77.3% of patients overall (88.3% among patients with urinary infection), regardless of first or second treatment line. In-hospital mortality rate was 23.1%. Adverse events were reported for six of the 569 patients enrolled.
This study provides important real-world evidence on treatment patterns, effectiveness, and safety of ceftazidime-avibactam in clinical practice through its recruitment in the European and LATAM regions. Ceftazidime-avibactam is one of the antibiotics to consider for treatment of MDR bacteria.
ClinicalTrials.gov identifier, NCT03923426.
在临床试验和真实世界研究中,头孢他啶-阿维巴坦已被证明对多重耐药(MDR)细菌具有活性。本研究旨在描述头孢他啶-阿维巴坦的使用模式(包括适应证和联合使用的抗生素),以及其在真实世界临床实践中的有效性和安全性。
这项非干预性病历回顾研究在欧洲和拉丁美洲(LATAM)地区的11个国家进行。纳入自2018年1月1日起(或该国上市日期,如更晚),在临床实践中因国家标签批准的适应证接受至少一剂头孢他啶-阿维巴坦治疗的连续患者。对接受头孢他啶-阿维巴坦治疗至少72小时的患者进行有效性分析。
在纳入的569例符合条件的患者中,516例(90.7%)接受了至少72小时的治疗(欧洲354例,拉丁美洲162例);390例患者(75.7%)从另一种用于革兰阴性菌覆盖的抗生素治疗方案转换而来。感染源包括腹腔内、泌尿系统、呼吸道、血流感染和其他感染(各约占20%)。肺炎克雷伯菌是开始使用头孢他啶-阿维巴坦前最新微生物评估中最常见的病原体(59.3%)。三分之二接受药敏试验的微生物为多重耐药菌,其中89.3%对碳青霉烯类耐药。肺炎克雷伯菌常见的多重耐药机制为碳青霉烯酶(33.9%)、氧青霉烷酶48(25.2%)、超广谱β-内酰胺酶(21.5%)或金属β-内酰胺酶(14.2%)的产生。在患者未预先接触过的情况下,17株分离菌(主要为肺炎克雷伯菌)对头孢他啶-阿维巴坦耐药。总体而言,77.3%的患者治疗成功(泌尿系统感染患者中为88.3%),无论为一线还是二线治疗。住院死亡率为23.1%。在纳入的569例患者中,有6例报告了不良事件。
本研究通过在欧洲和拉丁美洲地区的招募,提供了关于头孢他啶-阿维巴坦在临床实践中的治疗模式、有效性和安全性的重要真实世界证据。头孢他啶-阿维巴坦是治疗多重耐药菌时可考虑使用的抗生素之一。
ClinicalTrials.gov标识符,NCT03923426。