Division of Oncology, Mass General Cancer Center and Harvard Medical School, Boston, MA, USA.
Duke University School of Medicine, Durham, NC, USA.
Oncologist. 2023 Apr 6;28(4):341-350. doi: 10.1093/oncolo/oyac251.
Non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH) are the leading causes of hepatocellular carcinoma (HCC) worldwide. Limited data exist on surgical outcomes for NAFLD/NASH-related HCC compared with other HCC etiologies. We evaluated differences in clinicopathological characteristics and outcomes of patients undergoing surgical resection for NAFLD/NASH-associated HCC compared with other HCC etiologies.
Demographic, clinicopathological features, and survival outcomes of patients with surgically resected HCC were collected. NAFLD activity score (NAS) and fibrosis score were assessed by focused pathologic review in a subset of patients.
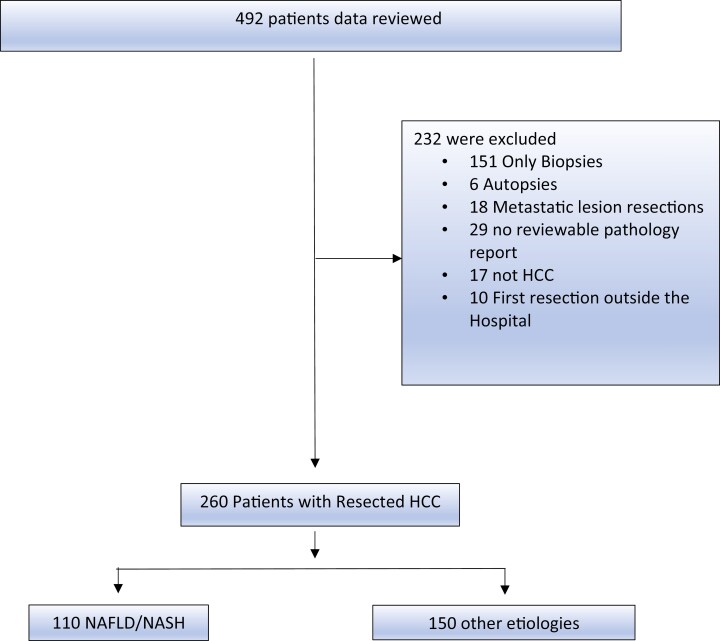
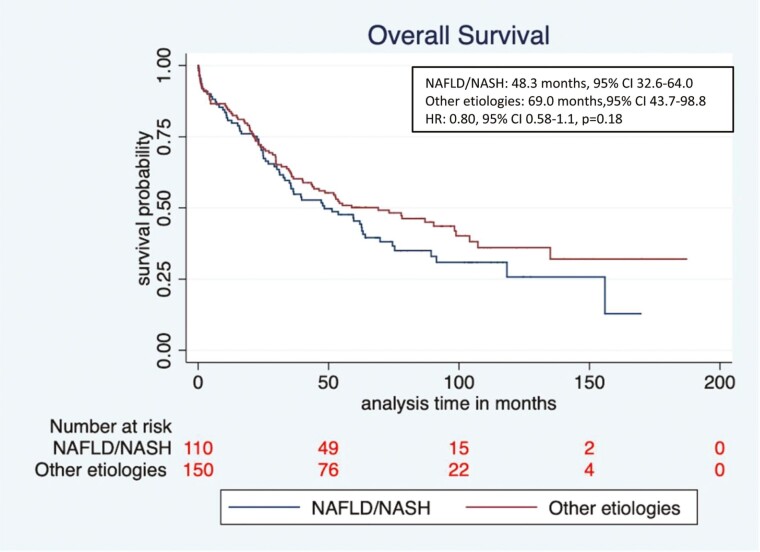
Among 492 patients screened, 260 met eligibility (NAFLD/NASH [n = 110], and other etiologies [n = 150]). Median age at diagnosis was higher in the NAFLD/NASH HCC cohort compared with the other etiologies cohort (66.7 vs. 63.4 years, respectively, P = .005), with an increased percentage of female patients (36% vs. 18%, P = .001). NAFLD/NASH-related tumors were more commonly >5 cm (66.0% vs. 45%, P = .001). There were no significant differences in rates of lymphovascular or perineural invasion, histologic grade, or serum AFP levels. The NAFLD/NASH cohort had lower rates of background liver fibrosis, lower AST and ALT levels, and higher platelet counts (P < .01 for all). Median overall survival (OS) was numerically shorter in NAFLD/NASH vs other etiology groups, however, not statistically significant.
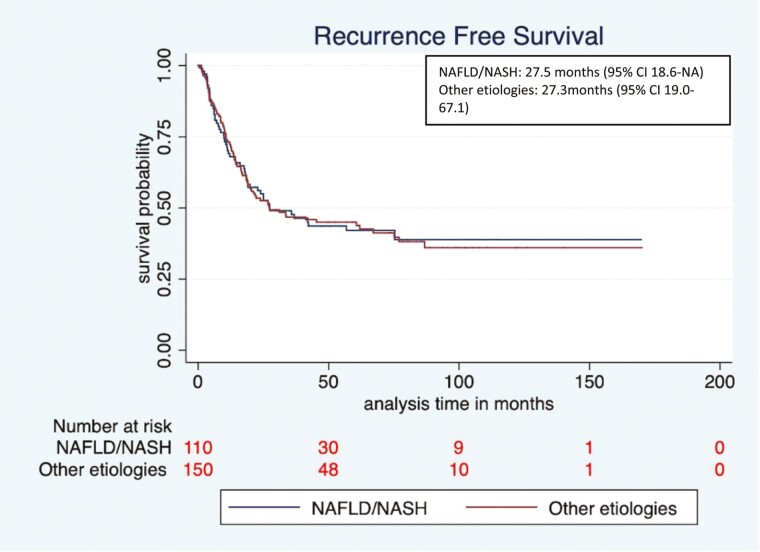
Patients with NAFLD/NASH-related HCC more commonly lacked liver fibrosis and presented with larger HCCs compared with patients with HCC from other etiologies. No differences were seen in rates of other high-risk features or survival. With the caveat of sample size and retrospective analysis, this supports a similar decision-making approach regarding surgical resection for NAFLD/NASH and other etiology-related HCCs.
非酒精性脂肪性肝病(NAFLD)和非酒精性脂肪性肝炎(NASH)是全球肝细胞癌(HCC)的主要病因。与其他 HCC 病因相比,NAFLD/NASH 相关 HCC 的手术治疗结局的相关数据有限。我们评估了与其他 HCC 病因相比,接受手术切除的 NAFLD/NASH 相关 HCC 患者的临床病理特征和结局的差异。
收集接受 HCC 手术切除患者的人口统计学、临床病理特征和生存结局数据。在部分患者中通过集中的病理检查评估 NAFLD 活动评分(NAS)和纤维化评分。
在筛选的 492 名患者中,有 260 名符合入选标准(NAFLD/NASH [n=110]和其他病因 [n=150])。NAFLD/NASH HCC 组的诊断时年龄中位数高于其他病因组(分别为 66.7 岁和 63.4 岁,P=0.005),女性患者的比例更高(36%比 18%,P=0.001)。NAFLD/NASH 相关肿瘤更常见>5cm(66.0%比 45%,P=0.001)。两组的脉管侵犯或神经周围侵犯、组织学分级或血清 AFP 水平无显著差异。NAFLD/NASH 组的背景肝纤维化率较低,AST 和 ALT 水平较低,血小板计数较高(所有 P<0.01)。NAFLD/NASH 组的总生存(OS)中位数略短,但无统计学意义。
与其他病因相关 HCC 患者相比,NAFLD/NASH 相关 HCC 患者更常见无肝纤维化且 HCC 更大。两组其他高危特征或生存情况无差异。鉴于样本量和回顾性分析的局限性,这支持对 NAFLD/NASH 和其他病因相关 HCC 患者的手术切除做出相似的决策。