Fujiwara Naoto, Nakagawa Hayato
Department of Gastroenterology and Hepatology, Graduate School of Medicine, Mie University, Tsu city, Japan.
Cancer Sci. 2023 Oct;114(10):3825-3833. doi: 10.1111/cas.15925. Epub 2023 Aug 7.
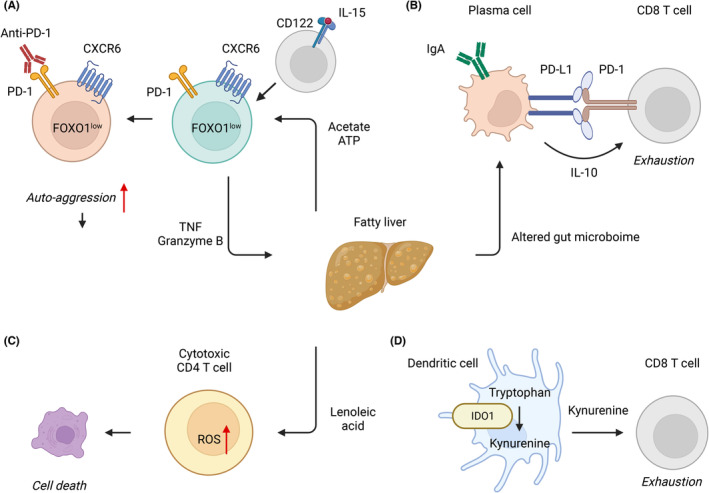
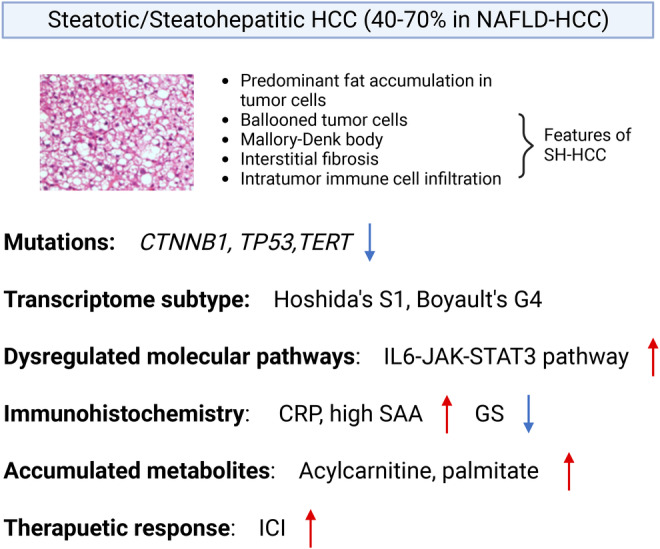
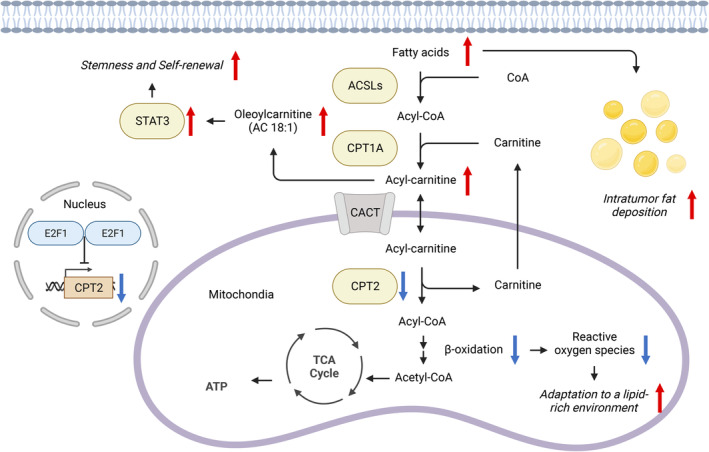
Patients with nonalcoholic fatty liver disease (NAFLD) continue to increase with the epidemics of obesity, and NAFLD is estimated to become the most prevalent etiology of hepatocellular carcinoma (HCC). Recently, NAFLD-HCC has been recognized to have clinico-histologically and molecularly distinct features from those from other etiologies, including a lower incidence rate of HCC and less therapeutic efficacy to immune checkpoint inhibitors (ICIs). Consistent with the clinical observations that up to 50% of NAFLD-HCC occurs in the absence of cirrhosis, the imbalance of pro- and antitumorigenic hepatic stellate cells termed as myHSC and cyHSC can contribute to the creation of an HCC-prone hepatic environment, independent of the absolute fibrosis abundance. Immune deregulations by accumulated metabolites in NAFLD-affected livers, such as a fatty-acid-induced loss of cytotoxic CD4 T cells serving for immune surveillance and "auto-aggressive" CXCR6+ CD8 T cells, may promote hepatocarcinogenesis and diminish therapeutic response to ICIs. Steatohepatitic HCC (SH-HCC), characterized by the presence of fat accumulation in tumor cells, ballooned tumor cells, Mallory-Denk body, interstitial fibrosis, and intratumor immune cell infiltration, may represent a metabolic reprogramming for adapting to a lipid-rich tumor microenvironment by downregulating CPT2 and leveraging its intermediates as an "oncometabolite." Genome-wide analyses suggested that SH-HCC may be more responsive to ICIs given its mutual exclusiveness with β-catenin mutation/activation that promotes immune evasion. Thus, further understanding of NAFLD-specific hepatocarcinogenesis and HCC would enable us to improve the current daily practice and eventually the prognoses of patients with NAFLD.
随着肥胖症的流行,非酒精性脂肪性肝病(NAFLD)患者数量持续增加,据估计NAFLD将成为肝细胞癌(HCC)最常见的病因。最近,人们认识到NAFLD-HCC在临床组织学和分子特征上与其他病因导致的HCC不同,包括HCC发病率较低以及对免疫检查点抑制剂(ICIs)的治疗效果较差。与临床观察结果一致,高达50%的NAFLD-HCC发生在无肝硬化的情况下,被称为肌成纤维细胞样肝星状细胞(myHSC)和静止性肝星状细胞(cyHSC)的促肿瘤和抗肿瘤肝星状细胞失衡可导致易发生HCC的肝脏环境的形成,而与绝对纤维化程度无关。NAFLD影响的肝脏中积累的代谢产物引起的免疫失调,如脂肪酸诱导的用于免疫监视的细胞毒性CD4 T细胞丧失和“自身攻击性”CXCR6+ CD8 T细胞,可能促进肝癌发生并降低对ICIs的治疗反应。脂肪性肝炎性肝癌(SH-HCC)的特征是肿瘤细胞中存在脂肪堆积、气球样变的肿瘤细胞、马洛里-登克小体、间质纤维化和肿瘤内免疫细胞浸润,可能代表通过下调肉碱棕榈酰转移酶2(CPT2)并利用其中间产物作为“肿瘤代谢物”来适应富含脂质的肿瘤微环境的代谢重编程。全基因组分析表明,SH-HCC可能对ICIs更敏感,因为它与促进免疫逃逸的β-连环蛋白突变/激活相互排斥。因此,进一步了解NAFLD特异性肝癌发生和HCC将使我们能够改善当前的日常实践,并最终改善NAFLD患者的预后。