Lin Ting-Yu, Chiu Sherry Yueh-Hsia, Liao Ling-Chun, Chen Sam Li-Sheng, Chiu Han-Mo, Chen Tony Hsiu-Hsi
Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, Taipei, Taiwan.
Department of Health Care Management, College of Management, Chang Gung University, Taoyuan, Taiwan.
NPJ Digit Med. 2023 Feb 10;6(1):24. doi: 10.1038/s41746-023-00763-5.
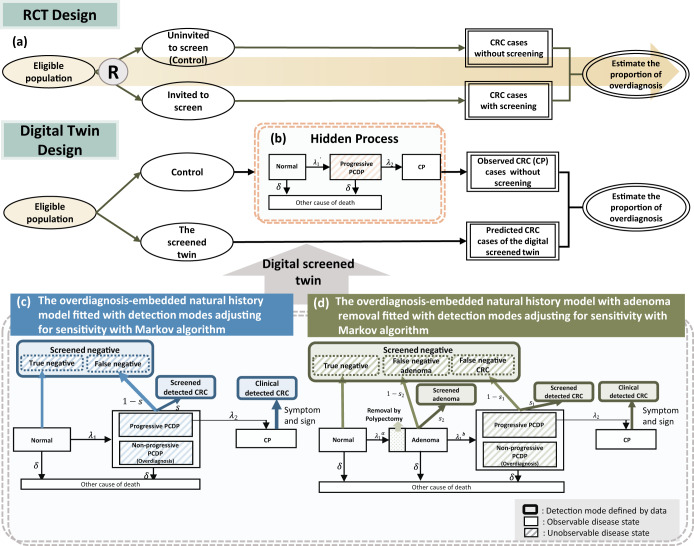
Evaluating the magnitude of overdiagnosis associated with stool-based service screening for colorectal cancer (CRC) beyond a randomized controlled trial is often intractable and understudied. We aim to estimate the proportion of overdiagnosis in population-based service screening programs for CRC with the fecal immunochemical test (FIT). The natural process of overdiagnosis-embedded disease was first built up to learn transition parameters that quantify the pathway of non-progressive and progressive screen-detected cases calibrated with sensitivity, while also taking competing mortality into account. The Markov algorithms were then developed for estimating these transition parameters based on Taiwan FIT service CRC screening data on 5,417,699 residents aged 50-69 years from 2004 to 2014. Following the digital twin design with the parallel universe structure for emulating the randomized controlled trial, the screened twin, mirroring the control group without screening, was virtually recreated by the application of the above-mentioned trained parameters to predict CRC cases containing overdiagnosis. The ratio of the predicted CRCs derived from the screened twin to the observed CRCs of the control group minus 1 was imputed to measure the extent of overdiagnosis. The extent of overdiagnosis for invasive CRCs resulting from FIT screening is 4.16% (95% CI: 2.61-5.78%). The corresponding figure is increased to 9.90% (95% CI: 8.41-11.42%) for including high grade dysplasia (HGD) and further inflated to 15.83% (95% CI: 15.23-16.46%) when the removal adenoma is considered. The modest proportion of overdiagnosis modelled by the digital twin method, dispensing with the randomized controlled trial design, suggests the harm done to population-based FIT service screening is negligible.
评估基于粪便检测的结直肠癌(CRC)筛查服务中过度诊断的程度,超出随机对照试验范围往往难以处理且研究不足。我们旨在估计基于人群的粪便免疫化学检测(FIT)CRC筛查项目中过度诊断的比例。首先构建了嵌入过度诊断疾病的自然过程,以了解过渡参数,这些参数量化了经灵敏度校准的非进展性和进展性筛查发现病例的途径,同时也考虑了竞争死亡率。然后基于2004年至2014年台湾5417699名50 - 69岁居民的FIT服务CRC筛查数据,开发了马尔可夫算法来估计这些过渡参数。按照具有平行宇宙结构的数字孪生设计来模拟随机对照试验,通过应用上述训练参数虚拟重建筛查孪生对象,该对象反映未进行筛查的对照组,以预测包含过度诊断的CRC病例。将筛查孪生对象预测的CRC病例数与对照组观察到的CRC病例数之比减去1,用于衡量过度诊断的程度。FIT筛查导致的浸润性CRC的过度诊断程度为4.16%(95%CI:2.61 - 5.78%)。当包括高级别上皮内瘤变(HGD)时,相应数字增至9.90%(95%CI:8.41 - 11.42%),若考虑切除腺瘤则进一步增至15.83%(95%CI:15.23 - 16.46%)。通过数字孪生方法模拟的适度过度诊断比例,无需随机对照试验设计,表明对基于人群的FIT服务筛查造成的危害可忽略不计。