Kaufmann Christoph C, Ahmed Amro, Muthspiel Marie, Rostocki Isabella, Pogran Edita, Zweiker David, Burger Achim Leo, Jäger Bernhard, Aicher Gabriele, Spiel Alexander O, Vafai-Tabrizi Florian, Gschwantler Michael, Fasching Peter, Wojta Johann, Huber Kurt
3rd Medical Department with Cardiology and Intensive Care Medicine, Klinik Ottakring (Wilhelminenhospital), 1160 Vienna, Austria.
Department of Endocrinology and Rheumatology, Klinik Ottakring (Wilhelminenhospital), 1160 Vienna, Austria.
J Clin Med. 2023 Jan 27;12(3):975. doi: 10.3390/jcm12030975.
Excess cardiovascular (CV) morbidity and mortality has been observed in patients with COVID-19. Both interleukin-32 (IL-32) and interleukin-34 (IL-34) have been hypothesized to contribute to CV involvement in COVID-19.
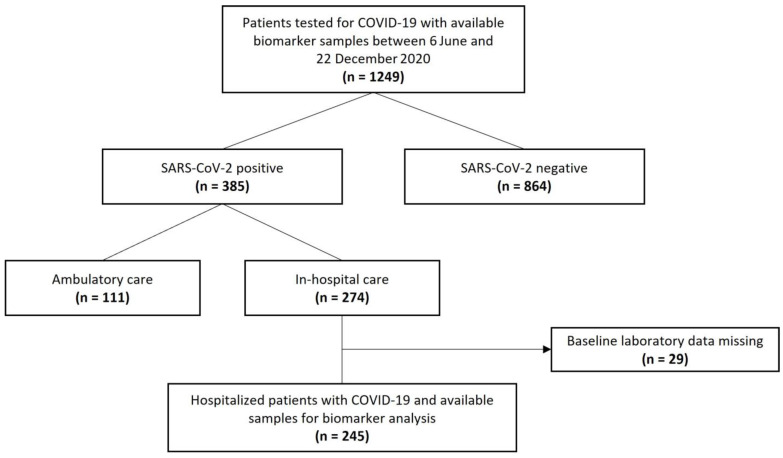
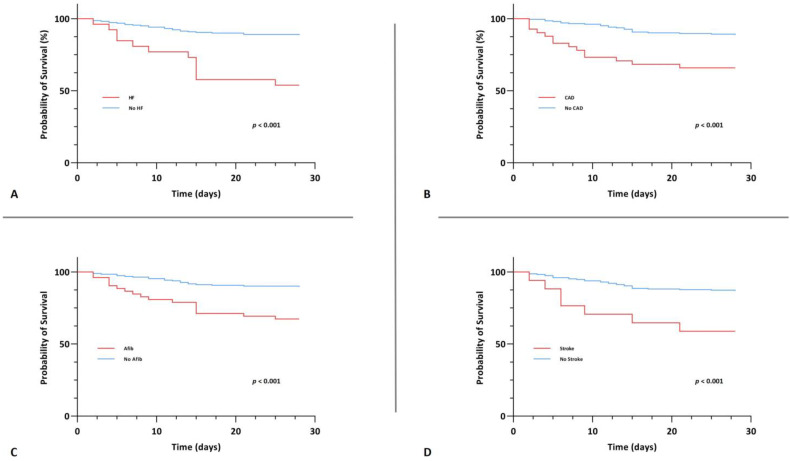
This prospective, observational study of patients with laboratory-confirmed COVID-19 infection was conducted from 6 June to 22 December 2020 in a tertiary care hospital in Vienna, Austria. IL-32 and IL-34 levels on admission were collected and tested for their association with CV disease and short-term mortality in patients with COVID-19. CV disease was defined by the presence of coronary artery disease, heart failure, stroke or atrial fibrillation and patients were stratified by CV disease burden.
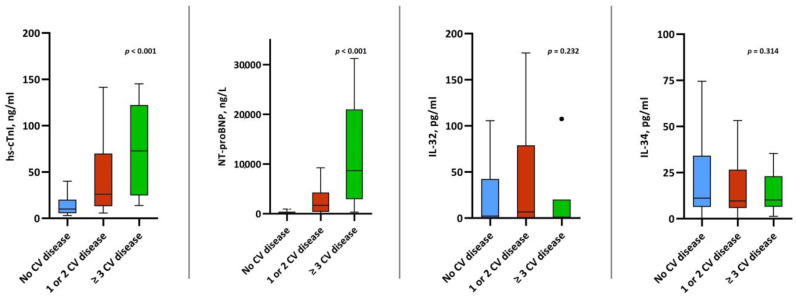
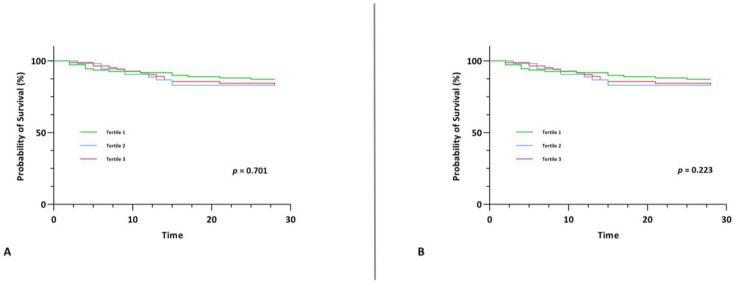
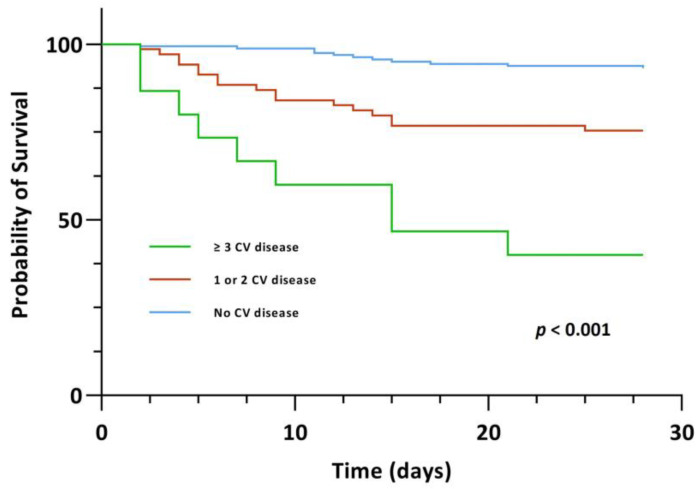
A total of 245 eligible patients with COVID-19 were included, of whom 37 (15.1%) reached the primary endpoint of 28-day mortality. Of the total sample, 161 had no CV disease (65.7%), 69 had one or two CV diseases (28.2%) and 15 patients had ≥three CV diseases (6.1%). Median levels of IL-32 and IL-34 at admission were comparable across the three groups of CV disease burden. IL-32 and IL-34 failed to predict mortality upon both univariable and multivariable Cox regression analysis. The two CV disease groups, however, had a significantly higher risk of mortality within 28 days (one or two CV diseases: crude HR 4.085 (95% CI, 1.913-8.725), < 0.001 and ≥three CV diseases: crude HR 13.173 (95% CI, 5.425-31.985), < 0.001). This association persisted for those with ≥three CV diseases after adjustment for age, gender and CV risk factors (adjusted HR 3.942 (95% CI, 1.288-12.068), = 0.016).
In our study population of hospitalized patients with COVID-19, IL-32 and IL-34 did not show any associations with CV disease or 28-day mortality in the context of COVID-19. Patients with multiple CV diseases, however, had a significantly increased risk of short-term mortality.
在新型冠状病毒肺炎(COVID-19)患者中观察到心血管(CV)发病率和死亡率过高。白细胞介素-32(IL-32)和白细胞介素-34(IL-34)均被认为与COVID-19患者的心血管受累有关。
2020年6月6日至12月22日,在奥地利维也纳的一家三级护理医院对实验室确诊的COVID-19感染患者进行了这项前瞻性观察研究。收集入院时的IL-32和IL-34水平,并检测其与COVID-19患者心血管疾病和短期死亡率的相关性。心血管疾病由冠状动脉疾病、心力衰竭、中风或心房颤动的存在来定义,患者按心血管疾病负担进行分层。
共纳入245例符合条件的COVID-19患者,其中37例(15.1%)达到28天死亡率的主要终点。在总样本中,161例无心血管疾病(65.7%),69例有一或两种心血管疾病(28.2%),15例有≥三种心血管疾病(6.1%)。三组心血管疾病负担患者入院时IL-32和IL-34的中位数水平相当。在单变量和多变量Cox回归分析中,IL-32和IL-34均未能预测死亡率。然而,这两组心血管疾病患者在28天内的死亡风险显著更高(一或两种心血管疾病:粗风险比(HR)4.085(95%置信区间(CI),1.913 - 8.725),P < 0.001;≥三种心血管疾病:粗HR 13.173(95% CI,5.425 - 31.985),P < 0.001)。在调整年龄、性别和心血管危险因素后,≥三种心血管疾病患者的这种关联仍然存在(调整后HR 3.942(95% CI,1.288 - 12.068),P = 0.016)。
在我们的住院COVID-19患者研究人群中,IL-32和IL-34在COVID-19背景下与心血管疾病或28天死亡率无任何关联。然而,患有多种心血管疾病的患者短期死亡风险显著增加。