Cherbi Miloud, Roubille François, Lamblin Nicolas, Bonello Laurent, Leurent Guillaume, Levy Bruno, Elbaz Meyer, Champion Sebastien, Lim Pascal, Schneider Francis, Cariou Alain, Khachab Hadi, Bourenne Jeremy, Seronde Marie-France, Schurtz Guillaume, Harbaoui Brahim, Vanzetto Gerald, Quentin Charlotte, Delabranche Xavier, Aissaoui Nadia, Combaret Nicolas, Tomasevic Danka, Marchandot Benjamin, Lattuca Benoit, Henry Patrick, Gerbaud Edouard, Bonnefoy Eric, Puymirat Etienne, Maury Philippe, Delmas Clément
Intensive Cardiac Care Unit, Rangueil University Hospital, Toulouse, France.
Institute of Metabolic and Cardiovascular Diseases (I2MC), UMR-1048, National Institute of Health and Medical Research (INSERM), Toulouse, France.
Front Cardiovasc Med. 2023 Jan 26;10:1092904. doi: 10.3389/fcvm.2023.1092904. eCollection 2023.
Cardiogenic shock (CS) is a life-threatening condition carrying poor prognosis, potentially triggered by ventricular arrhythmia (VA). Whether the occurrence of VA as trigger of CS worsens the prognosis compared to non-VA triggers remains unclear. The aim of this study was to evaluate 1-year outcomes [mortality, heart transplantation, ventricular assist devices (VAD)] between VA-triggered and non-VA-triggered CS.
FRENSHOCK is a prospective multicenter registry including 772 CS patients from 49 centers. One to three triggers can be identified in the registry (ischemic, mechanical complications, ventricular/supraventricular arrhythmia, bradycardia, iatrogenesis, infection, non-compliance). Baseline characteristics, management and 1-year outcomes were analyzed according to the VA-trigger in the CS population.
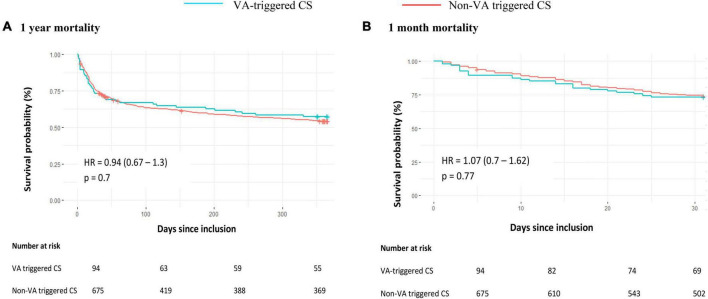
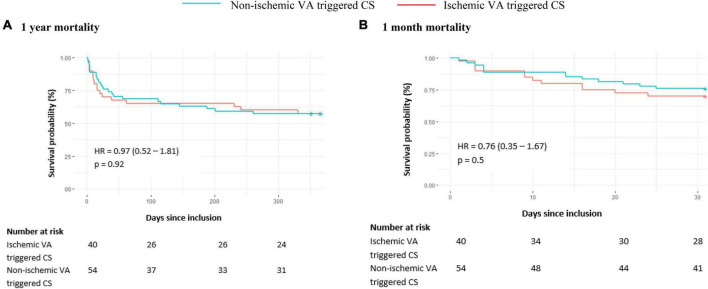
Within 769 CS patients included, 94 were VA-triggered (12.2%) and were compared to others. At 1 year, although there was no mortality difference [42.6 vs. 45.3%, HR 0.94 (0.67-1.30), = 0.7], VA-triggered CS resulted in more heart transplantations and VAD (17 vs. 9%, = 0.02). Into VA-triggered CS group, though there was no 1-year mortality difference between ischemic and non-ischemic cardiomyopathies [42.5 vs. 42.6%, HR 0.97 (0.52-1.81), = 0.92], non-ischemic cardiomyopathy led to more heart transplantations and VAD (25.9 vs. 5%, = 0.02).
VA-triggered CS did not show higher mortality compared to other triggers but resulted in more heart transplantation and VAD at 1 year, especially in non-ischemic cardiomyopathy, suggesting the need for earlier evaluation by advanced heart failure specialized team for a possible indication of mechanical circulatory support or heart transplantation.
https://clinicaltrials.gov, identifier NCT02703038.
心源性休克(CS)是一种危及生命且预后不良的疾病,可能由室性心律失常(VA)引发。与非VA引发的情况相比,VA作为CS的触发因素是否会使预后更差尚不清楚。本研究的目的是评估由VA引发和非VA引发的CS患者的1年结局[死亡率、心脏移植、心室辅助装置(VAD)]。
FRESHOCK是一项前瞻性多中心注册研究,纳入了来自49个中心的772例CS患者。在该注册研究中可确定一至三种触发因素(缺血、机械并发症、室性/室上性心律失常、心动过缓、医源性因素、感染、不依从)。根据CS人群中VA触发因素分析基线特征、治疗及1年结局。
在纳入的769例CS患者中,94例由VA触发(12.2%),并与其他患者进行比较。1年时,虽然死亡率无差异[42.6%对45.3%,风险比(HR)0.94(0.67 - 1.30),P = 0.7],但由VA触发的CS导致更多的心脏移植和VAD使用(17%对9%,P = 0.02)。在由VA触发的CS组中,虽然缺血性和非缺血性心肌病之间1年死亡率无差异[42.5%对42.6%,HR 0.97(0.52 - 1.81),P = 0.92],但非缺血性心肌病导致更多的心脏移植和VAD使用(25.9%对5%,P = 0.02)。
与其他触发因素相比,由VA触发的CS并未显示出更高的死亡率,但在1年时导致更多的心脏移植和VAD使用,尤其是在非缺血性心肌病中,这表明需要由晚期心力衰竭专科团队进行更早的评估,以确定是否可能需要机械循环支持或心脏移植。