Zeineddine Fadl A, Zeineddine Mohammad A, Yousef Abdelrahman, Gu Yue, Chowdhury Saikat, Dasari Arvind, Huey Ryan W, Johnson Benny, Kee Bryan, Lee Michael S, Morelli Maria Pia, Morris Van K, Overman Michael J, Parseghian Christine, Raghav Kanwal, Willis Jason, Wolff Robert A, Kawaguchi Yoshikuni, Vauthey Jean-Nicolas, Sun Ryan, Kopetz Scott, Shen John Paul
Department of Gastrointestinal Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Department of Surgical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
NPJ Precis Oncol. 2023 Feb 13;7(1):16. doi: 10.1038/s41698-023-00353-4.
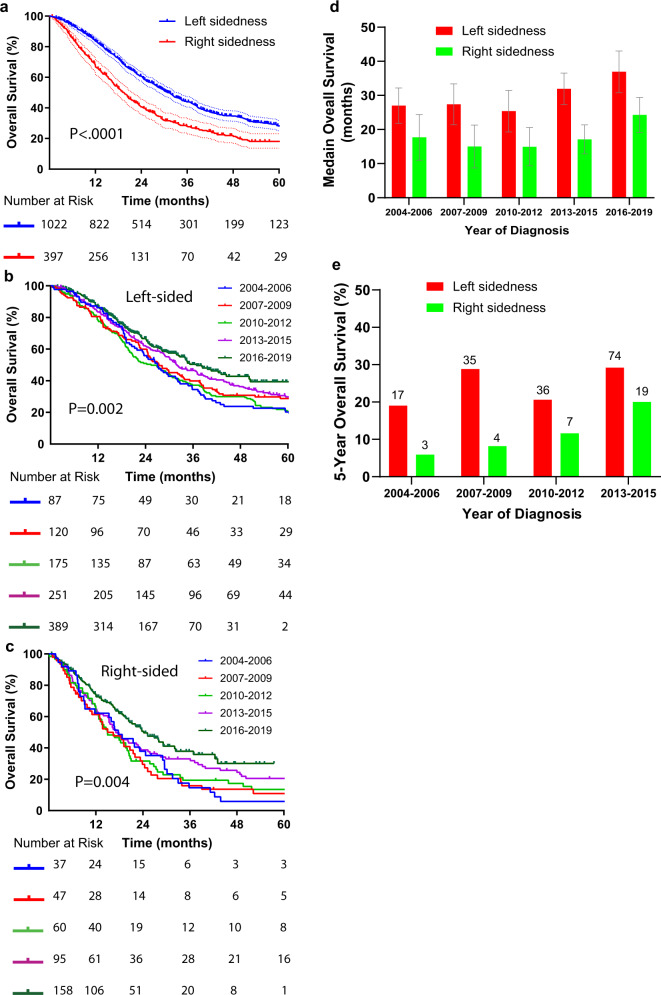
Over the past two decades of successive clinical trials in metastatic colorectal cancer (CRC), the median overall survival of both control and experimental arms has steadily improved. However, the incremental change in survival for metastatic CRC patients not treated on trial has not yet been quantified. We performed a retrospective review of 1420 patients with de novo metastatic CRC who received their primary treatment at the University of Texas M.D. Anderson Cancer Center (UTMDACC) from 2004 through 2019. Median OS was roughly stable for patients diagnosed between 2004 and 2012 (22.6 months) but since has steadily improved for those diagnosed in 2013 to 2015 (28.8 months), and 2016 to 2019 (32.4 months). Likewise, 5-year survival rate has increased from 15.7% for patients diagnosed from 2004 to 2006 to 26% for those diagnosed from 2013 to 2015. Notably, survival improved for patients with BRAF mutant as well as microsatellite unstable (MSI-H) tumors. Multivariate regression analysis identified surgical resection of liver metastasis (HR = 0.26, 95% CI, 0.19-0.37), use of immunotherapy (HR = 0.44, 95% CI, 0.29-0.67) and use of third line chemotherapy (regorafenib or trifluridine/tipiracil, HR = 0.74, 95% CI, 0.58-0.95), but not year of diagnosis (HR = 0.99, 95% CI, 0.98-1), as associated with better survival, suggesting that increased use of these therapies are the drivers of the observed improvement in survival.
在过去二十年针对转移性结直肠癌(CRC)的连续临床试验中,对照组和试验组的总生存期中位数均稳步提高。然而,未参与试验治疗的转移性CRC患者的生存增量变化尚未得到量化。我们对2004年至2019年在德克萨斯大学MD安德森癌症中心(UTMDACC)接受初始治疗的1420例初发性转移性CRC患者进行了回顾性研究。2004年至2012年诊断的患者的总生存期中位数大致稳定(22.6个月),但2013年至2015年诊断的患者(28.8个月)以及2016年至2019年诊断的患者(32.4个月)的总生存期中位数此后稳步提高。同样,5年生存率已从2004年至2006年诊断的患者的15.7%提高到2013年至2015年诊断的患者的26%。值得注意的是,携带BRAF突变以及微卫星不稳定(MSI-H)肿瘤的患者的生存率有所提高。多变量回归分析确定肝转移灶的手术切除(HR = 0.26,95% CI,0.19 - 0.37)、免疫疗法的使用(HR = 0.44,95% CI,0.29 - 0.67)以及三线化疗(瑞戈非尼或曲氟尿苷/替匹嘧啶,HR = 0.74,95% CI,0.58 - 0.95)与更好的生存率相关,但诊断年份(HR = 0.99,95% CI,0.98 - 1)与之无关,这表明这些疗法使用的增加是观察到的生存率提高的驱动因素。