Department of Gastroenterology, Renai branch, Taipei City Hospital, Taipei, Taiwan.
Department of Psychology, National Chengchi University, Taipei, Taiwan.
Clin Mol Hepatol. 2023 Jul;29(3):605-622. doi: 10.3350/cmh.2022.0342. Epub 2023 Feb 15.
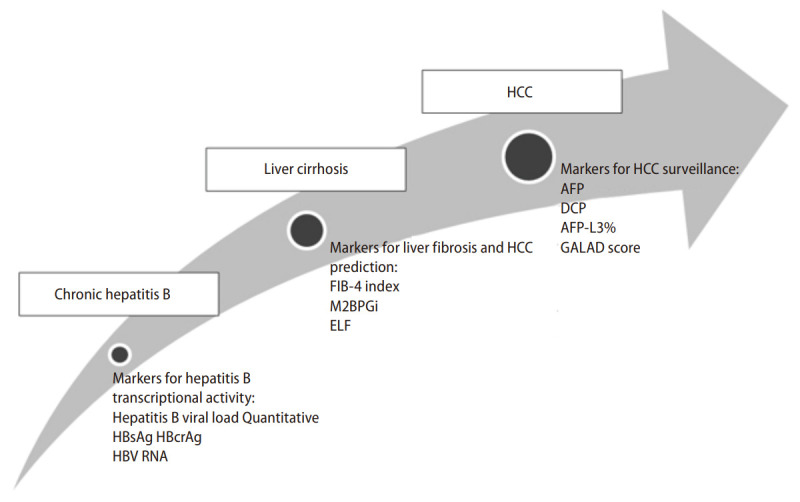
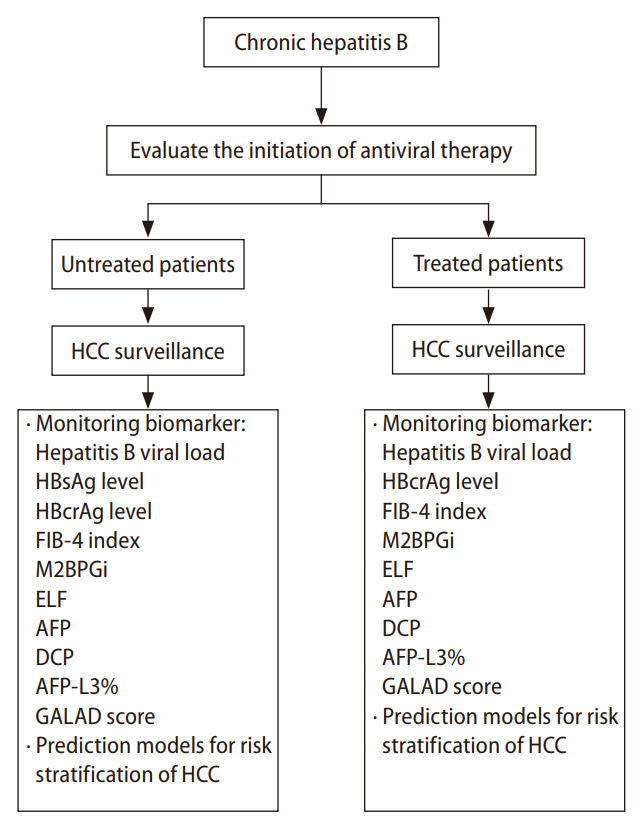
Hepatitis B virus (HBV) is responsible for more than 50% of hepatocellular carcinoma (HCC) in HBV hyperendemic areas, such as the Asia-Pacific region. Several hepatitis B viral factors are involved in HBV-related hepatocarcinogenesis. Hepatitis B viral load is the most important risk factor of HCC development. In addition, HBV integration, HBV genotype C, and core-promoter mutations are also associated with a risk of HCC development. For untreated chronic hepatitis B (CHB) patients, the estimated HCC incidence rates per 100 patient-years were 0.03-0.17 in inactive carriers, 0.07-0.42 in asymptomatic carriers, 0.12-0.49 in chronic hepatitis, and 2.03-3.37 in cirrhosis. Complementary to HBV DNA, serum levels of the hepatitis B surface antigen and hepatitis B core-related antigen (HBcrAg) can predict the occurrence of HCC for untreated patients with low and intermediate viral loads, respectively. For patients receiving antiviral therapy, the risks of HCC occurrence 40-60% lower than those for untreated patients. Patients treated with residual detectable HBV DNA or intrahepatic cccDNA still have a risk of HCC. Serum levels of HBcrAg, M2BPGi and fibrosis-4 are predictive of the risk of HCC development in treated patients. Several well-developed HCC risk scores can help clinicians identify high-risk CHB patients for HCC surveillance, regardless of treatment status. These strategies can help minimize the threat of HCC and prolong survival in CHB patients.
乙型肝炎病毒(HBV)是导致乙型肝炎病毒高流行地区(如亚太地区)超过 50%肝细胞癌(HCC)的主要原因。多种 HBV 病毒因素参与 HBV 相关的肝癌发生。HBV 病毒载量是 HCC 发展的最重要危险因素。此外,HBV 整合、HBV 基因型 C 和核心启动子突变也与 HCC 发展的风险相关。对于未经治疗的慢性乙型肝炎(CHB)患者,无活动型携带者、无症状携带者、慢性肝炎和肝硬化患者的 HCC 年发生率估计分别为 0.03-0.17/100 患者年、0.07-0.42/100 患者年、0.12-0.49/100 患者年和 2.03-3.37/100 患者年。除 HBV DNA 外,乙型肝炎表面抗原和乙型肝炎核心相关抗原(HBcrAg)的血清水平可分别预测低和中病毒载量未经治疗患者 HCC 的发生。对于接受抗病毒治疗的患者,HCC 发生的风险比未治疗患者低 40-60%。残留可检测到的 HBV DNA 或肝内 cccDNA 的患者仍有发生 HCC 的风险。HBcrAg、M2BPGi 和纤维化-4 血清水平可预测治疗患者 HCC 发生的风险。几种成熟的 HCC 风险评分可帮助临床医生识别高风险 CHB 患者,以进行 HCC 监测,无论治疗状况如何。这些策略有助于最大限度地降低 CHB 患者 HCC 的威胁并延长其生存时间。