AdventHealth for Children and AdventHealth Transplant Institute, Orlando, Florida, USA.
Helios University Hospital Wuppertal, Witten Herdecke University, Wuppertal, Germany.
Hepatol Commun. 2023 Feb 14;7(3):e0031. doi: 10.1097/HC9.0000000000000031. eCollection 2023 Mar 1.
Approximately 3.5 million children and adolescents worldwide are chronically infected with HCV. This study uses pharmacokinetic modeling to identify pediatric doses of elbasvir/grazoprevir (EBR/GZR) that achieve plasma concentrations similar to those seen in adults receiving the approved fixed-dose combination regimen of EBR/GZR.
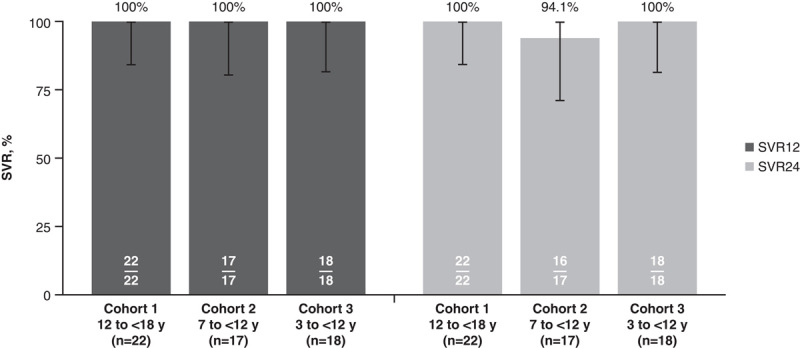
We conducted a nonrandomized, single-arm, multicenter, open-label phase 2b trial in children and adolescents aged 3 to <18 years with chronic HCV genotype 1 or 4 infection (NCT03379506). Pharmacokinetic data were used to bridge efficacy and safety data from adults to children in a stepwise (oldest to youngest) manner. A total of 57 participants were enrolled: cohort 1 (aged 12 to <18 y), n=22; cohort 2 (aged 7 to <12 y), n=17; and cohort 3 (aged 3 to <7 y), n=18.
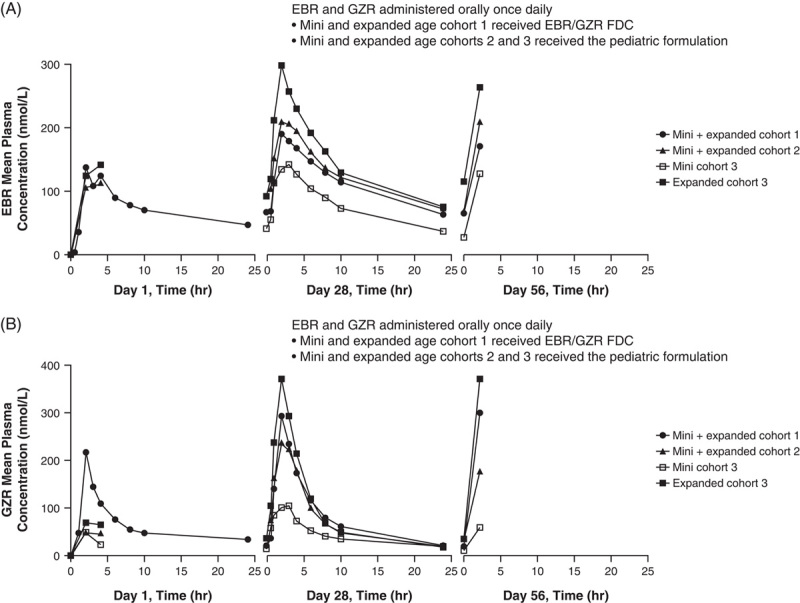
Steady-state plasma exposures were achieved by week 4 for EBR and GZR in all cohorts and daily dosing achieved geometric mean steady-state area under the concentration-time curve at 0-24 hours that fell within comparability bounds established for adults. All participants achieved sustained virologic response 12 weeks after completing treatment (ie, undetectable HCV RNA 12 wk following completion of treatment). Headache (n=4), fatigue (n=4), and nausea (n=2) were the most common treatment-related adverse events (all mild or moderate); no participant discontinued because of an adverse event.
Pediatric EBR/GZR pharmacokinetic models were successfully developed based on complex adult population pharmacokinetic models. At appropriate age-related doses, EBR/GZR is safe and effective in pediatric and adolescent participants with HCV infection.
全球约有 350 万儿童和青少年慢性感染 HCV。本研究采用药代动力学模型,确定了艾尔巴韦/格拉瑞韦(EBR/GZR)的儿科剂量,使血浆浓度与接受批准的 EBR/GZR 固定剂量组合方案的成人相似。
我们进行了一项非随机、单臂、多中心、开放标签的 2b 期临床试验,纳入了年龄在 3 至<18 岁的慢性 HCV 基因型 1 或 4 感染的儿童和青少年(NCT03379506)。药代动力学数据用于以逐步(从最年长到最年轻)的方式将成人的疗效和安全性数据外推至儿童。共纳入 57 名参与者:队列 1(年龄 12 至<18 岁),n=22;队列 2(年龄 7 至<12 岁),n=17;队列 3(年龄 3 至<7 岁),n=18。
所有队列在第 4 周时均达到 EBR 和 GZR 的稳态血浆暴露,每日剂量达到 0-24 小时的几何平均稳态浓度-时间曲线下面积,落在为成人建立的可比性范围内。所有参与者在完成治疗后 12 周时均达到持续病毒学应答(即,在完成治疗后 12 周时 HCV RNA 不可检测)。最常见的治疗相关不良事件是头痛(n=4)、疲劳(n=4)和恶心(n=2)(均为轻度或中度);无参与者因不良事件而停药。
根据复杂的成人群体药代动力学模型,成功建立了儿科 EBR/GZR 药代动力学模型。在适当的年龄相关剂量下,EBR/GZR 对 HCV 感染的儿科和青少年参与者是安全有效的。