Wu Yangyang, Lv Kaikai, Hao Xiaowei, Lv Chao, Lai Wenhui, Xia Xinze, Pang Aibo, Yuan Qing, Song Tao
Department of Urology, The Third Medical Centre, Chinese People's Liberation Army (PLA) General Hospital, Beijing, China.
Graduate School, Medical School of Chinese People's Liberation Army (PLA), Beijing, China.
Front Surg. 2023 Jan 30;10:1045363. doi: 10.3389/fsurg.2023.1045363. eCollection 2023.
Racial/ethnic disparity in waiting-list mortality among candidates listed for kidney transplantation (KT) in the United States remains unclear. We aimed to assess racial/ethnic disparity in waiting-list prognosis among patients listed for KT in the United States in the current era.
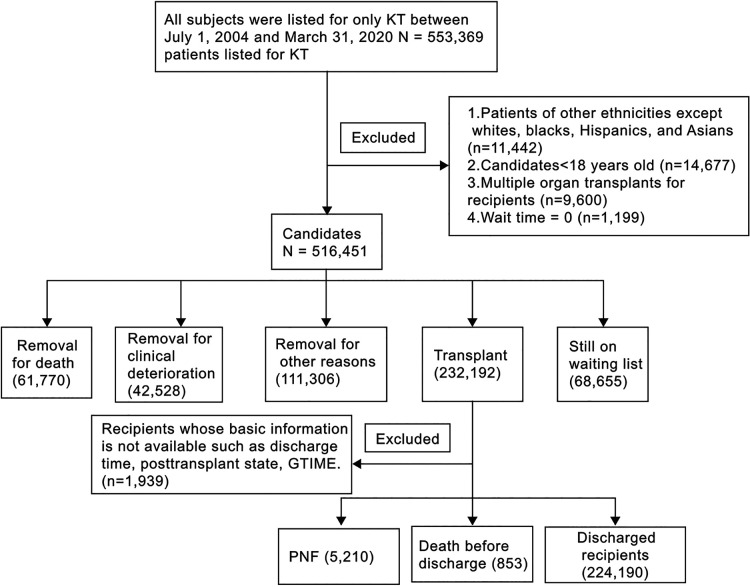
We compared waiting-list and early posttransplant in-hospital mortality or primary nonfunction (PNF) among adult (age ≥18 years) white, black, Hispanic, and Asian patients listed for only KT in the United States between July 1, 2004 and March 31, 2020.
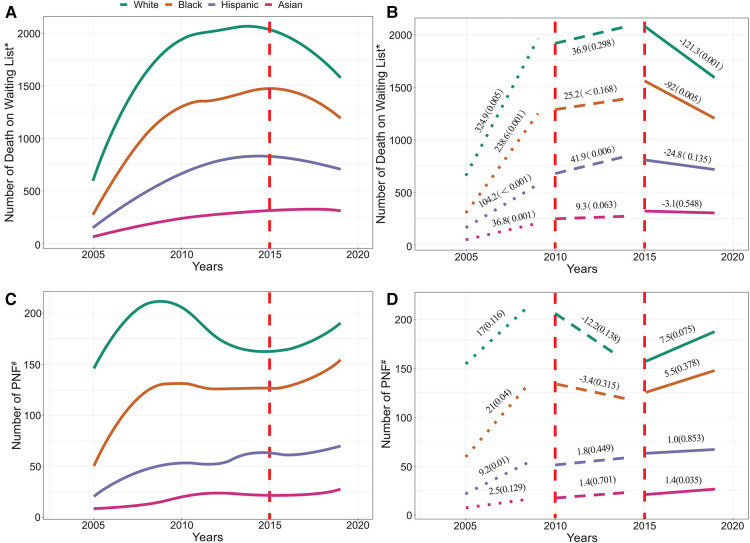
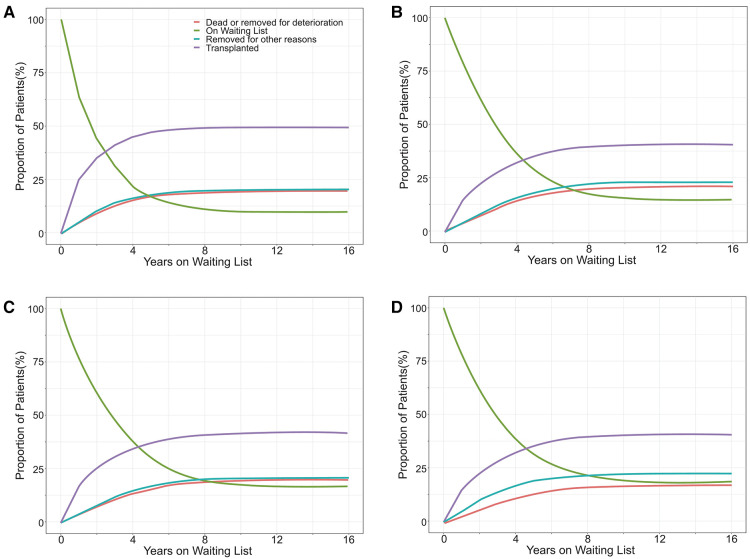
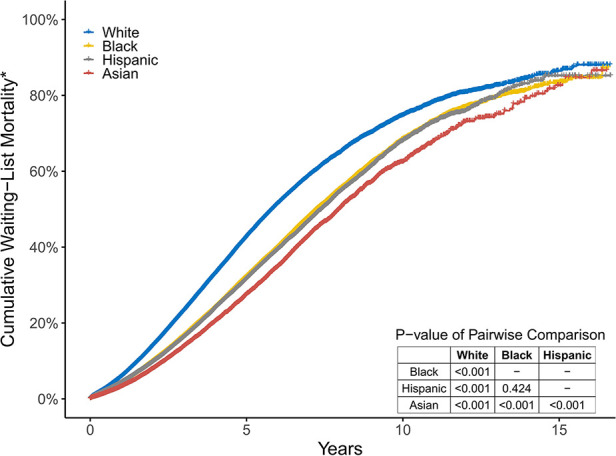
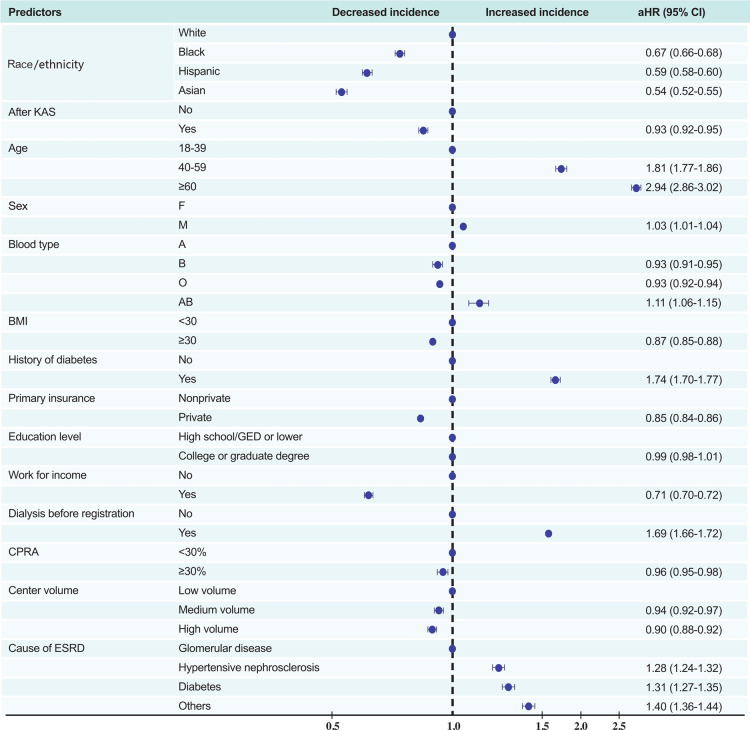
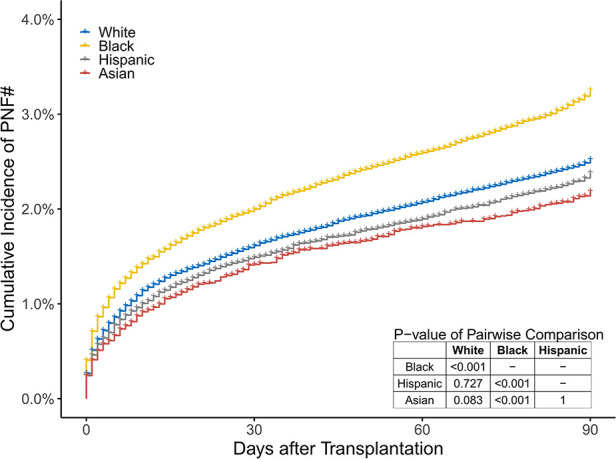
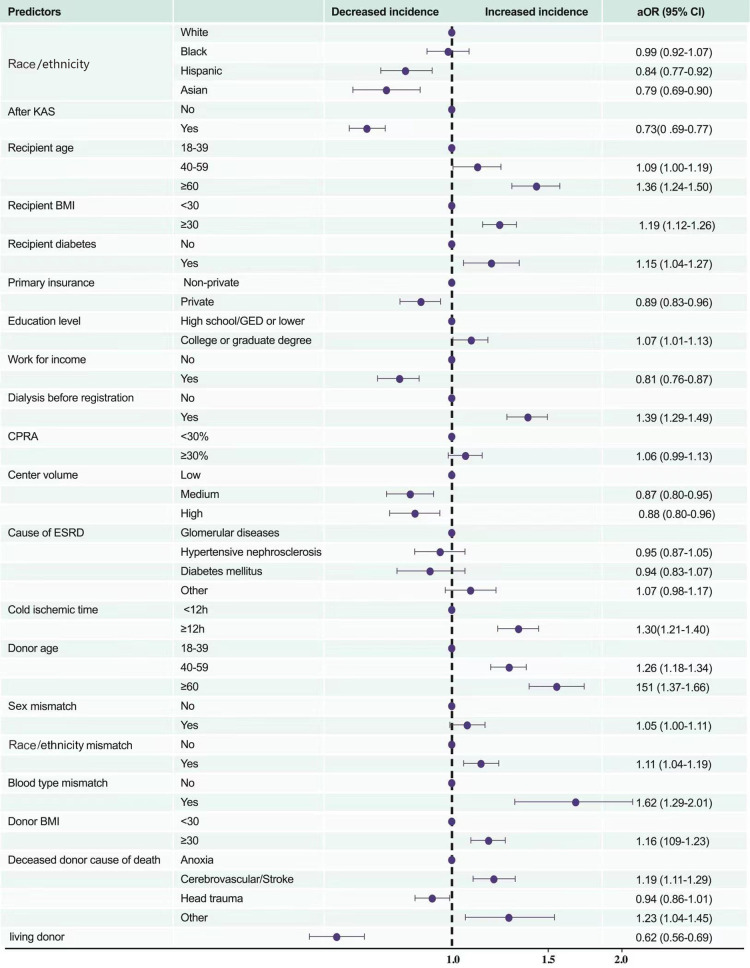
Of the 516,451 participants, 45.6%, 29.8%, 17.5%, and 7.1% were white, black, Hispanic, and Asian, respectively. Mortality on the 3-year waiting list (including patients who were removed for deterioration) was 23.2%, 16.6%, 16.2%, and 13.8% in white, black, Hispanic, and Asian patients, respectively. The cumulative incidence of posttransplant in-hospital death or PNF after KT was 3.3%, 2.5%, 2.4%, and 2.2% in black, white, Hispanic, and Asian patients,respectively. White candidates had the highest mortality risk on the waiting list or of becoming too sick for a transplant, while black (adjusted hazard ratio, [95% confidence interval, CI], 0.67 [0.66-0.68]), Hispanic (0.59 [0.58-0.60]), and Asian (0.54 [0.52-0.55]) candidates had a lower risk. Black KT recipients (odds ratio, [95% CI] 1.29 [1.21-1.38]) had a higher risk of PNF or death before discharge than white patients. After controlling confounders, black recipients (0.99 [0.92-1.07]) had a similar higher risk of posttransplant in-hospital mortality or PNF as white patients than Hispanic and Asian counterparts.
Despite having a better socioeconomic status and being allocated better kidneys, white patients had the worst prognosis during the waiting periods. Black recipients and white recipients have higher posttransplant in-hospital mortality or PNF.
在美国,等待肾移植(KT)的候选人中,种族/族裔在等待名单上的死亡率差异尚不清楚。我们旨在评估当前时代美国等待KT的患者在等待名单上的预后的种族/族裔差异。
我们比较了2004年7月1日至2020年3月31日期间仅在美国等待KT的成年(年龄≥18岁)白人、黑人、西班牙裔和亚洲患者在等待名单上以及移植后早期住院期间的死亡率或原发性无功能(PNF)情况。
在516,451名参与者中,分别有45.6%、29.8%、17.5%和7.1%为白人、黑人、西班牙裔和亚洲人。白人、黑人、西班牙裔和亚洲患者在3年等待名单上的死亡率(包括因病情恶化被移除的患者)分别为23.2%、16.6%、16.2%和13.8%。肾移植后住院死亡或PNF的累积发生率在黑人、白人、西班牙裔和亚洲患者中分别为3.3%、2.5%、2.4%和2.2%。白人候选人在等待名单上的死亡风险最高,或者因病情过重而无法进行移植,而黑人(调整后的风险比,[95%置信区间,CI],0.67[0.66 - 0.68])、西班牙裔(0.59[0.58 - 0.60])和亚洲(0.54[0.52 - 0.55])候选人的风险较低。黑人肾移植受者(优势比,[95%CI]1.29[1.21 - 1.38])在出院前发生PNF或死亡的风险高于白人患者。在控制混杂因素后,黑人受者(0.99[0.92 - 1.07])与白人患者相比,移植后住院死亡率或PNF的风险较高,高于西班牙裔和亚洲受者。
尽管白人患者社会经济地位较好且分配到更好的肾脏,但在等待期间预后最差。黑人受者和白人受者移植后住院死亡率或PNF较高。