Jiang Wen-Jing, Sun Zhen-Gao, Song Jing-Yan
The First Clinical College, Shandong University of Traditional Chinese Medicine, Jinan, China.
Reproductive Center of Integrated Medicine, The Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, China.
Heliyon. 2023 Jan 24;9(2):e13218. doi: 10.1016/j.heliyon.2023.e13218. eCollection 2023 Feb.
In a modified natural cycle frozen-thawed embryo transfer (mNC-FET), does the premature timing of progesterone luteal phase support (LPS) initiation 24 h following human chorionic gonadotropin (hCG) trigger impact live birth?
Premature LPS initiation did not negatively affect the live birth rate (LBR) in mNC-FET cycles compared with conventional LPS initiation 48 h after hCG triggering.
During natural cycle FET, human chorionic gonadotropin is routinely used to mimic endogenous luteinizing hormone (LH) surge to induce ovulation, which allows more flexibility in embryo transfer scheduling, thus relieving the burden of multiple visits by patients and laboratory workloads, which is also known as mNC-FET. Moreover, recent data demonstrates that ovulatory women undergoing natural cycle FETs have a lower risk of maternal and fetal complications due to the essential role of the corpus luteum in implantation, placentation and pregnancy maintenance. While several studies have confirmed the positive effects of LPS in mNC-FETs, the timing of progesterone LPS initiation is still unclear, as compared with fresh cycles where robust research has been conducted. To the best of our knowledge, no clinical studies comparing different beginning days in mNC-FET cycles have been published.
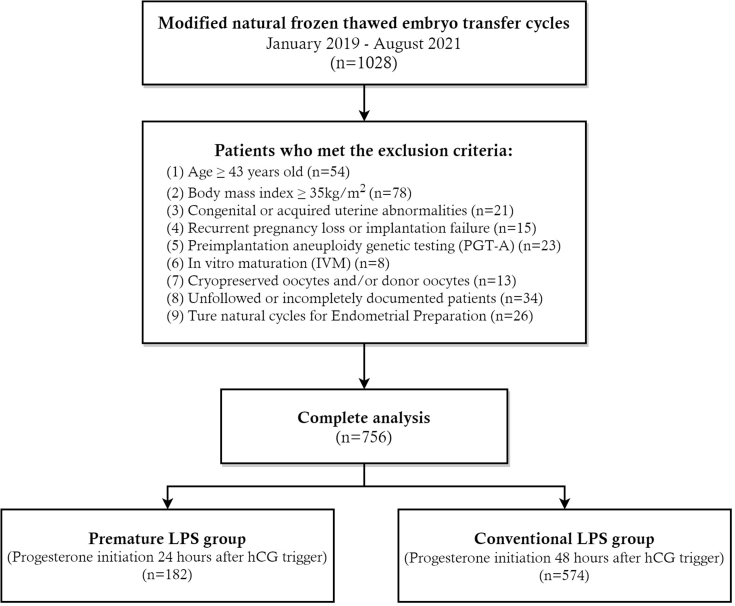
This retrospective cohort study involved 756 mNC-FET cycles performed at a university-affiliated reproductive center between January 2019 and August 2021. The primary outcome measured was the LBR.
PARTICIPANTS/MATERIALS SETTING METHODS: Ovulatory women ≤42 years of age who were referred for their autologous mNC-FET cycles were included in the study. According to the timing of progesterone LPS initiation following the hCG trigger, patients were assigned into two categories: premature LPS group (progesterone initiation 24 h after hCG trigger, n = 182) versus conventional LPS group (progesterone initiation 48 h after hCG trigger, n = 574). Multivariate logistic regression analysis was used to control for confounding variables.
There were no differences in background characteristics between the two study groups, except for the proportion of assisted hatching (53.8% in premature LPS group versus 42.3% in conventional LPS group, p = 0.007). In the premature LPS group, 56 of 182 patients (30.8%) had a live birth, compared to 179 of 574 patients (31.2%) in the conventional LPS group, with no significant difference observed between groups (adjusted odds ratio [aOR] 0.98, 95% confidence interval [CI] 0.67-1.43, p = 0.913). In addition, there was no significant difference between the two groups in other secondary outcomes. A sensitivity analysis for LBR according to the serum LH and progesterone levels on hCG trigger day also confirmed the aforementioned findings.
In this study, retrospective analysis was conducted in a single center and was therefore prone to bias. Additionally, we did not anticipate monitoring the patient's follicle rupture and ovulation after hCG triggering. Future prospective clinical trials remain necessary to confirm our results.
While exogenous progesterone LPS was added 24 h after hCG triggering, embryo-endometrium synchrony would not be adversely affected so long as sufficient time was allowed for endometrial exposure to exogenous progesterone. Our data support promising clinical outcomes following this event. As a result of our findings, clinicians and patients will be able to make better informed decisions.
STUDY FUNDING/COMPETING INTERESTS: No specific funding was available for this study. The authors have no personal conflicting interests to declare.
N/A.
在改良自然周期冻融胚胎移植(mNC-FET)中,人绒毛膜促性腺激素(hCG)触发后24小时开始黄体期孕酮支持(LPS)的时机过早是否会影响活产率?
与hCG触发后48小时开始常规LPS相比,过早开始LPS对mNC-FET周期的活产率(LBR)没有负面影响。
在自然周期FET中,人绒毛膜促性腺激素通常用于模拟内源性促黄体生成素(LH)激增以诱导排卵,这使得胚胎移植安排更加灵活,从而减轻了患者多次就诊的负担和实验室工作量,这也被称为mNC-FET。此外,最近的数据表明,由于黄体在着床、胎盘形成和维持妊娠中的重要作用,接受自然周期FET的排卵女性发生母婴并发症的风险较低。虽然多项研究证实了LPS在mNC-FET中的积极作用,但与已进行大量研究的新鲜周期相比,孕酮LPS开始的时机仍不清楚。据我们所知,尚未发表比较mNC-FET周期中不同开始日期的临床研究。
这项回顾性队列研究涉及2019年1月至2021年8月在一家大学附属生殖中心进行的756个mNC-FET周期。测量的主要结果是LBR。
参与者/材料设置方法:纳入年龄≤42岁、因自体mNC-FET周期前来就诊的排卵女性。根据hCG触发后开始黄体期孕酮支持的时间,将患者分为两类:过早LPS组(hCG触发后24小时开始使用孕酮,n = 182)与常规LPS组(hCG触发后48小时开始使用孕酮,n = 574)。采用多因素逻辑回归分析来控制混杂变量。
除辅助孵化比例外,两组的背景特征无差异(过早LPS组为53.8%,常规LPS组为42.3%,p = 0.007)。过早LPS组182例患者中有56例(30.8%)活产,常规LPS组574例患者中有179例(31.2%)活产,两组间无显著差异(调整优势比[aOR] 0.98,95%置信区间[CI] 0.67 - 1.43,p = 0.913)。此外,两组在其他次要结果方面也无显著差异。根据hCG触发日的血清LH和孕酮水平对LBR进行的敏感性分析也证实了上述发现。
在本研究中,在单一中心进行回顾性分析,因此容易产生偏差。此外,我们没有预期监测hCG触发后患者的卵泡破裂和排卵情况。未来仍有必要进行前瞻性临床试验以证实我们的结果。
虽然在hCG触发后24小时添加了外源性黄体期孕酮支持,但只要给予子宫内膜足够的时间暴露于外源性孕酮,胚胎 - 子宫内膜同步性就不会受到不利影响。我们的数据支持这一事件后有良好的临床结果。基于我们的研究结果,临床医生和患者将能够做出更明智的决策。
研究资金/利益冲突:本研究没有特定资金支持。作者没有个人利益冲突需要声明。
无。