From the Universitair Ziekenhuis Brussel (UZ Brussel) (G.P., G.N., M.D.), Department of Neurology, Belgium; Nationaal Multiple Sclerose Centrum (NMSC) (G.P., A.V.R., M.D.), Melsbroek, Belgium; Vrije Universiteit Brussel (VUB) (G.N., J.V.S., M.D.), Center for Neurosciences (C4N), NEUR and AIMS, Brussels, Belgium; Icometrix (G.N.), Leuven, Belgium; and Vrije Universiteit Brussel (VUB) (J.V.S.), Department of Electronics and Informatics (ETRO), Belgium.
Neurol Neuroimmunol Neuroinflamm. 2023 Feb 17;10(3). doi: 10.1212/NXI.0000000000200089. Print 2023 May.
Large-scale observational studies have shown that, in patients with multiple sclerosis (MS), the risk of becoming more severely ill from coronavirus disease 2019 (COVID-19) is determined by older age, male sex, cardiovascular comorbidities, African American ethnicity, progressive disease, recent use of corticosteroids, and B cell-depleting disease-modifying treatment. In contrast, the effect of COVID-19 on the disease course of MS has been studied much less extensively. Our main goal was to explore whether COVID-19 is associated with accelerated clinical disability worsening in patients with MS.
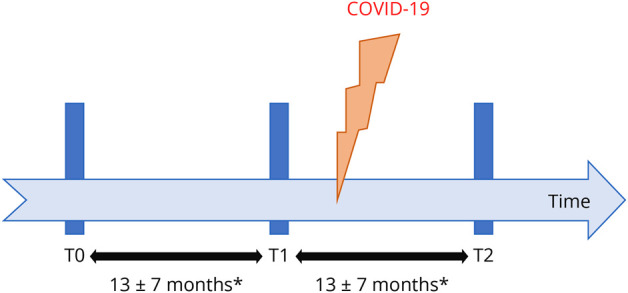
Since March 2020, demographics and infectious outcome (categorized as ambulatory, hospitalized, and/or death) of patients with MS who developed COVID-19 have been collected at the Belgian National MS Center in Melsbroek. On February 28, 2022, this database was locked and complemented with clinical disability measures-Expanded Disability Status Scale (EDSS), Timed 25-Foot Walk Test (T25FWT), 9-Hole Peg Test (9HPT), and Symbol Digit Modalities Test (SDMT)-that were available from a larger local database, obtained during routine medical follow-up. For each parameter, the first 2 assessments before COVID-19 diagnosis (T0 and T1; T1 is the closest to COVID-19 diagnosis), and the first thereafter (T2), were retrieved.
We identified 234 unique cases of COVID-19. Thirty-one patients were hospitalized (13.2%), and 5 died (2.1%) as a result of their infection. Among survivors with complete EDSS results (N = 138), mean annualized T1-to-T2 EDSS worsening was more pronounced, compared with the respective change between T0 and T1 (0.3 ± 0.9 vs 0.1 ± 0.9, = 0.012). No such differences were found for the T25FWT, 9HPT, and SDMT scores. Severe COVID-19 (hospitalization) was associated with clinically relevant T1-to-T2 EDSS worsening (OR 2.65, = 0.042). Vaccination coverage in the total cohort was 53.8%. Being unprotected by vaccination at the time of infection was associated with a worse COVID-19 outcome (hospitalization and/or death; OR 3.52, = 0.002) but not with clinically relevant T1-to-T2 EDSS worsening.
The occurrence and severity of COVID-19 are both associated with clinical disability worsening in patients with MS. Vaccination protects against a more severe course of COVID-19 in this specific population.
The study has been registered at ClinicalTrials.gov (study registration number: NCT05403463).
大型观察性研究表明,在多发性硬化症(MS)患者中,COVID-19 患病风险取决于年龄较大、男性、心血管合并症、非裔美国人种族、进行性疾病、近期使用皮质类固醇和 B 细胞耗竭性疾病修饰治疗。相比之下,COVID-19 对 MS 疾病过程的影响研究得要少得多。我们的主要目标是探讨 COVID-19 是否与 MS 患者的临床残疾恶化加速有关。
自 2020 年 3 月以来,在比利时 Melsbroek 的国家多发性硬化症中心收集了患有 MS 并发生 COVID-19 的患者的人口统计学和感染结果(分为门诊、住院和/或死亡)。2022 年 2 月 28 日,该数据库被锁定,并补充了从更大的本地数据库中获得的临床残疾测量值-扩展残疾状况量表(EDSS)、定时 25 英尺步行测试(T25FWT)、9 孔钉测试(9HPT)和符号数字模态测试(SDMT)。对于每个参数,都检索了 COVID-19 诊断前的前 2 次评估(T0 和 T1;T1 是距离 COVID-19 诊断最近的一次)和之后的第 1 次评估(T2)。
我们确定了 234 例 COVID-19 确诊病例。31 例患者住院(13.2%),5 例患者死亡(2.1%)。在幸存者中(N=138),完全有 EDSS 结果的患者 T1 到 T2 的 EDSS 恶化程度比 T0 到 T1 的变化更明显,分别为 0.3±0.9 比 0.1±0.9, =0.012)。T25FWT、9HPT 和 SDMT 评分则没有这种差异。严重的 COVID-19(住院)与临床相关的 T1 到 T2 的 EDSS 恶化有关(OR 2.65, =0.042)。总队列中的疫苗接种覆盖率为 53.8%。在感染时未接种疫苗的人,其 COVID-19 结局(住院和/或死亡)更差(OR 3.52, =0.002),但与临床相关的 T1 到 T2 的 EDSS 恶化无关。
COVID-19 的发生和严重程度都与 MS 患者的临床残疾恶化有关。疫苗接种可预防该特定人群 COVID-19 更严重的发病。
该研究已在 ClinicalTrials.gov 上注册(研究注册号:NCT05403463)。