Khanna Ashish K, Kinoshita Takahiro, Natarajan Annamalai, Schwager Emma, Linn Dustin D, Dong Junzi, Ghosh Erina, Vicario Francesco, Maheshwari Kamal
Department of Anesthesiology, Section on Critical Care Medicine, Wake Forest School of Medicine, Atrium Health Wake Forest Baptist Medical Center, Perioperative Outcomes and Informatics Collaborative, Winston-Salem, NC, 27106, USA.
Outcomes Research Consortium, Cleveland, OH, 44195, USA.
Ann Intensive Care. 2023 Feb 20;13(1):9. doi: 10.1186/s13613-023-01101-4.
Intensivists target different blood pressure component values to manage intensive care unit (ICU) patients with sepsis. We aimed to evaluate the relationship between individual blood pressure components and organ dysfunction in critically ill septic patients.
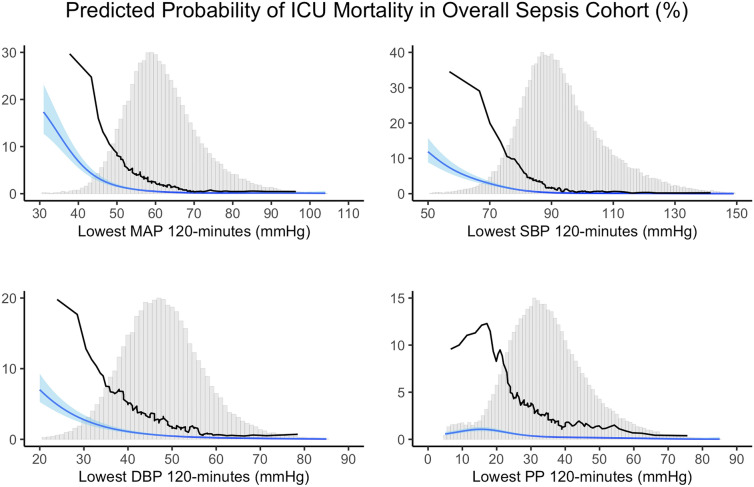
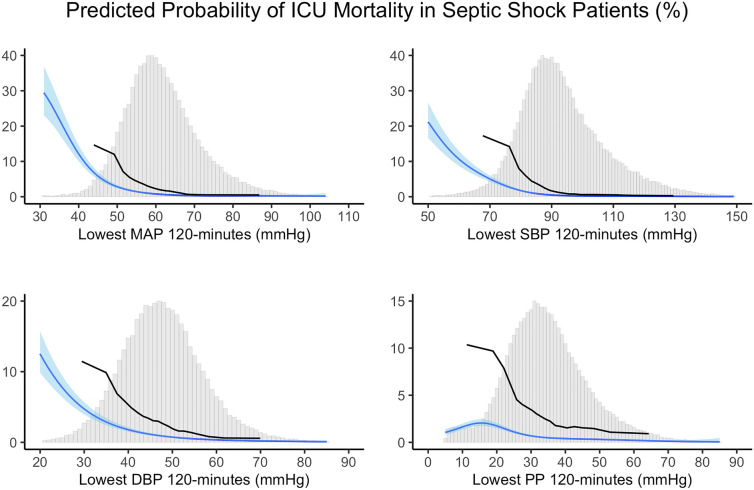
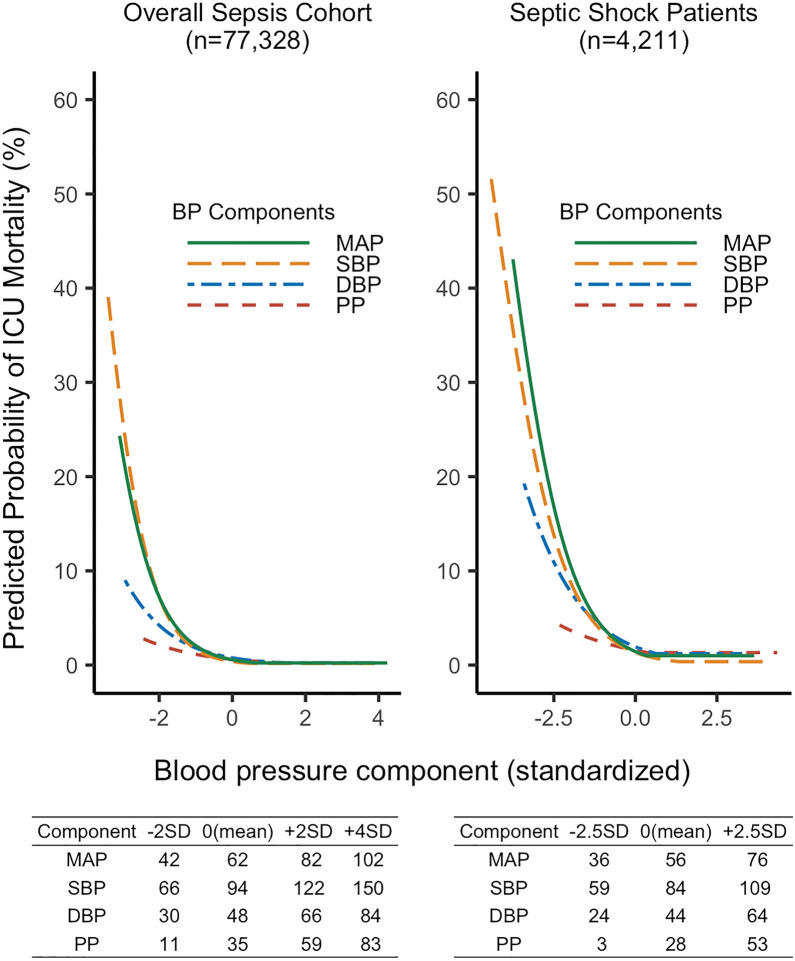
In this retrospective observational study, we evaluated 77,328 septic patients in 364 ICUs in the eICU Research Institute database. Primary exposure was the lowest cumulative value of each component; mean, systolic, diastolic, and pulse pressure, sustained for at least 120 min during ICU stay. Primary outcome was ICU mortality and secondary outcomes were composite outcomes of acute kidney injury or death and myocardial injury or death during ICU stay. Multivariable logistic regression spline and threshold regression adjusting for potential confounders were conducted to evaluate associations between exposures and outcomes. Sensitivity analysis was conducted in 4211 patients with septic shock.
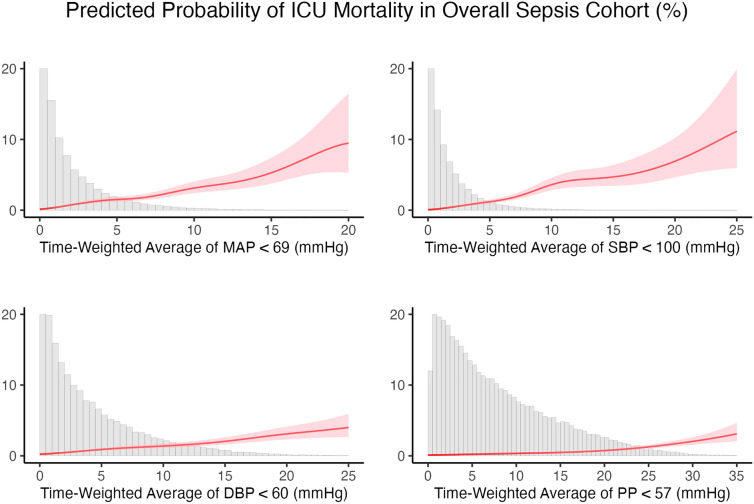
Lower values of all blood pressures components were associated with a higher risk of ICU mortality. Estimated change-points for the risk of ICU mortality were 69 mmHg for mean, 100 mmHg for systolic, 60 mmHg for diastolic, and 57 mmHg for pulse pressure. The strength of association between blood pressure components and ICU mortality as determined by slopes of threshold regression were mean (- 0.13), systolic (- 0.11), diastolic (- 0.09), and pulse pressure (- 0.05). Equivalent non-linear associations between blood pressure components and ICU mortality were confirmed in septic shock patients. We observed a similar relationship between blood pressure components and secondary outcomes.
Blood pressure component association with ICU mortality is the strongest for mean followed by systolic, diastolic, and weakest for pulse pressure. Critical care teams should continue to follow MAP-based resuscitation, though exploratory analysis focusing on blood pressure components in different sepsis phenotypes in critically ill ICU patients is needed.
重症监护医生针对不同的血压组成部分数值来管理脓毒症的重症监护病房(ICU)患者。我们旨在评估危重症脓毒症患者个体血压组成部分与器官功能障碍之间的关系。
在这项回顾性观察研究中,我们评估了电子ICU研究所数据库中364个ICU的77328例脓毒症患者。主要暴露因素是每个组成部分的最低累积值;平均压、收缩压、舒张压和脉压,在ICU住院期间持续至少120分钟。主要结局是ICU死亡率,次要结局是ICU住院期间急性肾损伤或死亡以及心肌损伤或死亡的复合结局。进行多变量逻辑回归样条分析和针对潜在混杂因素进行阈值回归分析,以评估暴露因素与结局之间的关联。对4211例脓毒症休克患者进行了敏感性分析。
所有血压组成部分的较低数值都与ICU死亡率较高风险相关。ICU死亡率风险的估计变化点为平均压69mmHg、收缩压100mmHg、舒张压60mmHg和脉压57mmHg。通过阈值回归斜率确定的血压组成部分与ICU死亡率之间的关联强度为平均压(-0.13)、收缩压(-0.11)、舒张压(-0.09)和脉压(-0.05)。在脓毒症休克患者中证实了血压组成部分与ICU死亡率之间存在等效的非线性关联。我们观察到血压组成部分与次要结局之间存在类似关系。
血压组成部分与ICU死亡率的关联中,平均压最强,其次是收缩压、舒张压,脉压最弱。重症监护团队应继续遵循基于平均动脉压的复苏方案,不过需要对危重症ICU患者不同脓毒症表型的血压组成部分进行探索性分析。